Respiratory Compromise
Published (updated: ).

A patient who is experiencing respiratory distress can develop respiratory compromise. It is the goal of the EMS crew to delay or reverse respiratory compromise. Failure reverse respiratory compromise will result in respiratory failure.
Exactly when the patient transitions to respiratory compromise from respiratory distress is not entirely defined, however some changes in the function and structure of the respiratory system are common:
- The residual pressure in the lungs increase, as does the surface area of the lungs. This increase in pressure effects gas exchange in the pulmonary capillary beds.
- The increased pressure and larger size of the lungs increase the pressure in the pleural lining. This increased pressure often causes some of the bronchioles to collapse, resulting in even less airflow.
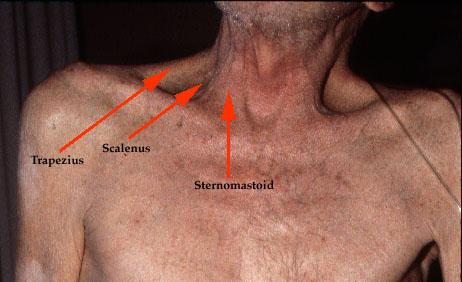
- In addition to the intercostal muscles and diaphragm, accessory muscles will be recruited to assist in moving air. It is easy to see accessory muscles by looking at the chest and neck. Intercostal retractions are due to reduced air pressure inside your chest. This can happen if the upper airway (trachea) or small airways of the lungs (bronchioles) become partially blocked. As a result, the intercostal muscles are sucked inward, between the ribs, when you breathe.
Inhalation is an active process, meaning the brain has to tell the ribcage to expand. The intercostals and diaphragm contract, causing the lungs to be stretched outwardly, decreasing the pressure inside the lungs causing air to fill the new vacuum (created by the stretched out lungs). In respiratory compromise, this balance of air pressure shifts towards the lungs having higher residual pressure. This means less air will be able to move in and out of the lungs with each breath.
Exhalation is a passive process, meaning the brain just tells the muscles of respiration to relax and the ribs (taking the lungs with it) become smaller, causing increased pressure in the lungs as compared with the environment. The air leaves the lungs and exits out of the mouth and nose.
