Congestive Heart Failure
Published (updated: ).
Introduction
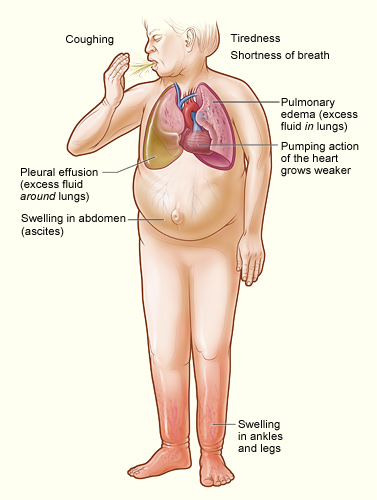
Heart failure is a complex clinical syndrome that results from a functional or structural heart disorder impairing ventricular filling or ejection of blood to the systemic circulation. It is by definition a failure to meet the systemic demands of circulation. Heart failure remains a highly prevalent disorder worldwide with a high morbidity and mortality rate. It has an estimated prevalence of 26 million people worldwide and contributes to increased healthcare costs worldwide. Multiple different diseases can cause heart failure. The etiology of heart failure varies the treatment plan to some degree; however, most of the treatment recommendations are based on the presence of heart failure alone, regardless of the cause.
Etiology
Congestive heart failure is caused by structural abnormalities of the heart, functional abnormalities, and other triggering factors. Historically, an overwhelming majority of the cases were due to coronary artery disease and myocardial infarction. Over time, coronary artery disease and diabetes mellitus have become the predominant predisposing factors for heart failure. Other structural causes of congestive heart failure (CHF) include hypertension, valvular heart disease, uncontrolled arrhythmia, myocarditis, and congenital heart disease. Diastolic heart failure with impaired ventricular filling can be caused by restrictive cardiomyopathies and constrictive pericarditis, in addition to the etiologies identified above.
It is important to identify etiologies of decompensated heart failure, as they contribute to most of the morbidity and mortality associated with the disease. The most common cause of decompensated congestive heart failure is inappropriate drug treatment, dietary sodium restriction, and decreased physical activity. Uncontrolled hypertension is the second most common cause of decompensated heart failure. Uncontrolled tachyarrhythmias in patients with underlying congestive heart failure can promptly lead to CHF exacerbations.
Another group of diseases associated with “congestive heart failure” leads to high-output cardiac failure. This, by definition, is not an impairment in cardiac function but a failure of the heart to meet the increased systemic demands due to extracardiac diseases. Common etiologies of this type of congestive heart failure include severe anemia, thyrotoxicosis, obesity, nutritional deficiencies (thiamine deficiency, etc.), and pregnancy.
Epidemiology
Approximately 6.2 million people in the United States had clinically manifested heart failure from 2013 to 2016. By some reports, the incidence rate has plateaued; however, the prevalence increases as more patients receive therapy. This has not translated to improved quality of life or a decrease in the number of hospitalizations for patients with heart failure. Age is a major determinant of HF. Regardless of the cause or the definition used to classify patients with heart failure (HF), the prevalence of HF increases steeply with age.
Pathophysiology
The adaptive mechanisms that may be adequate to maintain the overall contractile performance of the heart at relatively normal levels become maladaptive when trying to sustain adequate cardiac performance.
In the initial stages of congestive heart failure, cardiac physiology attempts to adapt via several compensatory mechanisms to maintain cardiac output and meet the systemic demands. These include the Frank-Starling mechanism, changes in myocyte regeneration, myocardial hypertrophy, and myocardial hypercontractility. With increased wall stress, the myocardium attempts to compensate via eccentric remodeling, which further worsens the loading conditions and wall stress.
A decrease in cardiac output stimulates the neuroendocrine system with a release of epinephrine, norepinephrine, endothelin-1 (ET-1), and vasopressin. They cause vasoconstriction leading to increased afterload. This increases myocardial contractility and further prevents myocardial relaxation.
An increase in afterload and myocardial contractility with impaired myocardial relaxation leads to increased myocardial oxygen demand. This paradoxical need for increased cardiac output to meet myocardial demand eventually leads to myocardial cell death and apoptosis. As apoptosis continues, a decrease in cardiac output with increased demand leads to a perpetuating cycle of increased neurohumoral stimulation and maladaptive hemodynamic and myocardial responses.
