Unstable Facial Fractures
Published (updated: ).
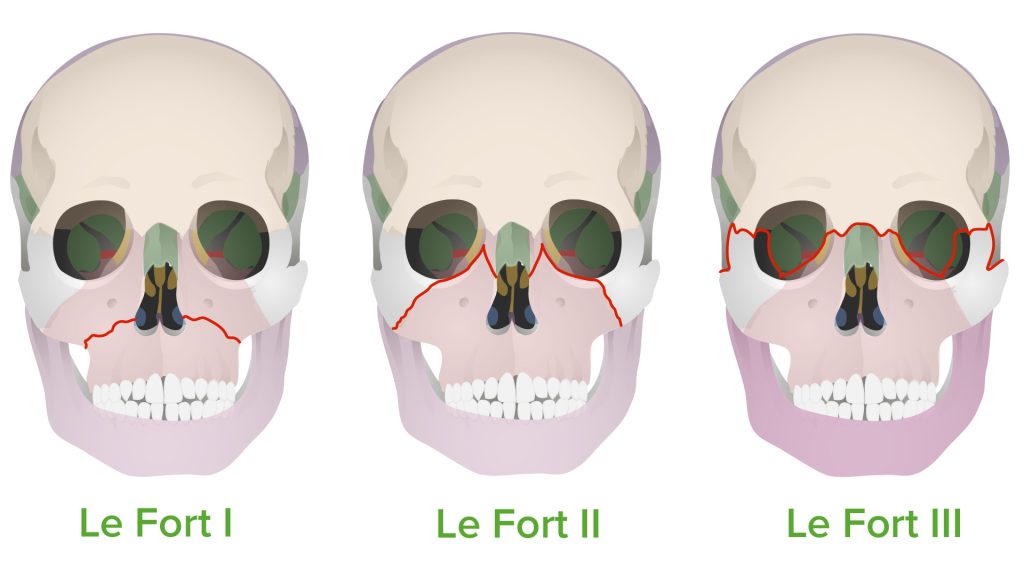
Le Fort injuries are complex fractures of the midface, named after Rene Le Fort who studied cadaver skulls that were subjected to blunt force trauma. His experiments determined the areas of structural weakness of the maxilla designated as “lines of weakness” where fractures occurred. These fractures are classified into 3 distinct groups based on the direction of the fracture: horizontal, pyramidal or transverse. The pterygoid plate is involved in all types of Le Fort fractures. This may result in a pterygomaxillary separation. The absence of a pterygoid fracture rules out a Le Fort fracture. However, the presence of a pterygoid fracture does not specifically indicate whether a Le Fort fracture exists. Up to one-third of pterygoid plate fractures do not result from a Le Fort fracture pattern.
Etiology
A high percentage of facial injuries occur secondary to injuries, from sports such as football, baseball, and hockey. Le Fort fractures can also occur secondary to motor vehicle collisions, assault, and fall from a substantial height. Patients with Le Fort fractures often have associated head and cervical spine injuries.
- Le Fort type I fractures may result from a force directed in a downward direction against the upper teeth.
- Le Fort type II fractures result from a force to lower or mid maxilla.
- Le Fort type III fractures are caused by impact to the nasal bridge and upper part of the maxilla
Epidemiology
Le Fort fractures account for 10% to 20% of all facial fractures. These may be potentially life-threatening and disfiguring in patients in whom the injury is significant.
Pathophysiology
Le Fort injuries occur with high-impact force when energy transfer to the body exceeds the tolerance of impacted tissue. Beware that these complex injuries seldom occur in isolation and are often associated with concomitant or life-threatening injuries.
Type of Fractures
Le Fort Type I
These fractures (trans-maxillary fracture) result from a force directed low on the maxillary rim in a downward direction. This occurs in the horizontal plane at the level of the base of the nose. A direct blow to the lower face causes fractures that involve all 3 walls of the maxillary sinus and pterygoid processes. The fracture extends around both maxillary antra, through the nasal septum and the pterygoid plates. This causes palate-facial separation. However, this fracture does not involve the glabella or zygoma.
Le Fort Type II
This pyramidal fracture occurs due to trauma to the midface. The fracture line begins in the region of the bridge of the nose (nasion) and extends obliquely through the medial aspect of the orbits and inferior orbital rims. It then continues posteriorly in a horizontal fashion above the hard palate to involve the pterygomaxillary buttresses, resulting in a disarticulation of the pyramid-shaped facial skeleton from the remainder of the skull. Note that the zygoma remains attached to the cranium.
Le Fort Type III
Also called cranial-facial separation, the fracture line in this injury passes from the nasofrontal area across the medial, posterior, and lateral orbital walls, the zygomatic arch, and through the upper portion of pterygoid plates.
Anatomic Level Classification
Le Fort Type I
Transverse fracture through the maxilla above the roots of the teeth, separating teeth from the upper face. These can be unilateral or bilateral.
Le Fort Type II
These fractures extend superiorly in the midface to include the nasal bridge, maxilla, lacrimal bones, orbital floor, and rim. They are pyramidal fractures with teeth at the base and nasal bone at the apex. These fractures are typically bilateral.
Le Fort Type III
This type of fracture starts at the bridge of the nose and extends posteriorly along the medial wall of the orbit and the floor of the orbit, and then through the lateral orbital wall and the zygomatic arch. The fractures run parallel with the base of the skull, separating the entire midfacial skeleton from the cranial base. This discontinuity between the skull and the face is termed craniofacial dissociation. This may be associated with a cerebrospinal fluid (CSF) leak.
Causes
Le Fort Type I
These fractures result from a force directed low on the maxillary rim in a downward direction. Fractures extend from the nasal septum to lateral pyriform rims, and extend horizontally above the teeth, crossing below the zygomaxillary junction, then traversing the pterygomaxillary junction interrupting the pterygoid plates.
Le Fort Type II
These fractures result from a force to the lower or mid maxilla. This fracture has a pyramidal shape and extends from the nasal bridge at the nasofrontal suture through the maxilla. Inferolaterally, the fracture extends through the lacrimal bone and inferior orbital floor near the inferior orbital foramen and inferiorly through the anterior wall of the maxillary sinus. On the lateral aspect, it travels under the zygoma, across the pterygomaxillary fissure, and through the pterygoid plate.
Le Fort Type III
These fractures result from an impact to the nasal bridge or upper maxilla. This results in complete craniofacial disjunction.
History and Physical
Presentation
Le Fort Type I
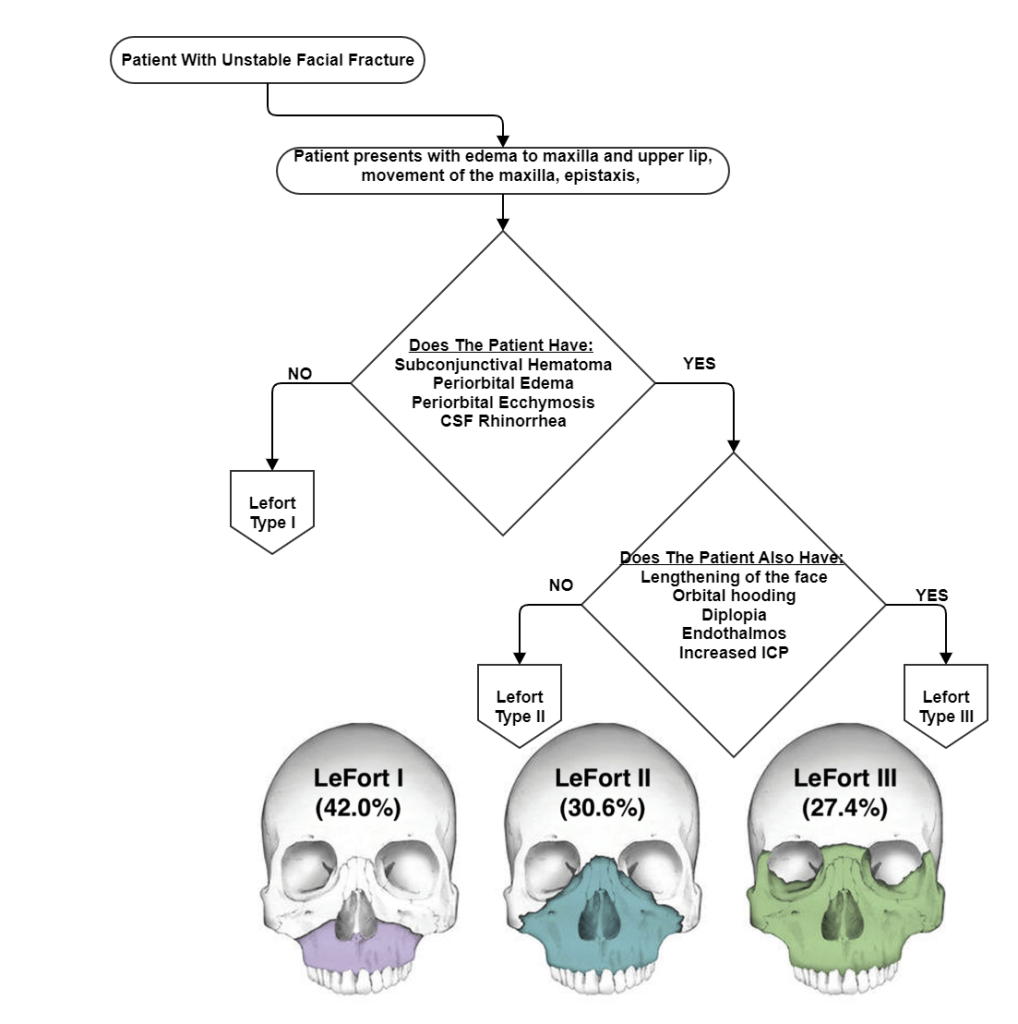
Le Fort type I presents as a swollen upper lip, anterior open bite malocclusion, ecchymosis of the maxillary buccal vestibule and palate, and mobility of the maxilla.
Le Fo rt Type II
With a Le Fort type II fracture, there is significant deformity and swelling, widening of the intercanthal space (nasal septum fracture), mobility of the maxilla and nose as a combined segment, as well as bilateral periorbital edema and ecchymosis (raccoon eyes), epistaxis, anterior open bite malocclusion, ecchymosis of the maxillary buccal vestibule and palate, and possible CSF rhinorrhea. Since the fracture involves the inferior orbital rim and floor, there may be sensory deficits in the infraorbital region extending inferiorly to the upper lip.
Le Fo rt Type III
The most significant clinical findings are demonstrated by bilateral periorbital edema and ecchymosis (raccoon eyes), ecchymosis of the maxillary buccal vestibule and palate, lengthening of facial height- elongation and flattening of the face (dish-face deformity), orbital hooding, enophthalmos, ecchymosis over the mastoid region (Battle’s sign), CSF rhinorrhea, CSF otorrhea, and hemotympanum.
Evaluation
The primary survey includes airway and cervical spine stabilization, breathing and ventilatory support, attention to circulation and hemorrhage control, disability and neurologic evaluation, and exposure and environment control.
Airway obstruction associated with fractures of the midfacial skeleton can be life-threatening if not recognized promptly and treated appropriately. Orotracheal intubation is required when intranasal damage is a possibility. Airway obstruction in Le Fort injuries mainly occurs due to multiple sources bleeding into the upper airway, as well as midface altered airway anatomy. Beware that the risk of life-threatening hemorrhage in Le Fort II and III injuries is higher than that associated with other facial injuries.
Maxillofacial trauma is an obvious threat to the patient’s airway; therefore, a rapid evaluation must be performed to determine the need for a definitive airway. The concept of the definitive airway in cases of maxillofacial trauma is probably much more critical as compared to trauma to other body parts; therefore, an emergency airway may be required.
In a patient with complex maxillofacial trauma, cervical spine fracture should always be considered unless proven otherwise. Therefore, the cervical spine must be protected while providing airway management.
During the secondary survey, the assessment of maxillofacial fractures is performed after initial stabilization and resuscitation of the multisystem trauma patient. An ophthalmologic evaluation is required in Le Fort II and III fractures with orbital involvement. This should be completed before surgery to ensure there is no globe injury.
The mobility of the face should be tested on both sides as well as in the midline. The type of Le Fort fracture is determined by which regions are mobile.
- Le Fort I: Mobility of the maxilla; maxilla is free from the rest of the facial bones (floating palate)
- Le Fort II: Mobility of the maxilla and nose as a combined segment
- Le Fort III: Mobilized segment to include the maxilla, nose, and zygomas
A CT scan of facial bones is required to fully and adequately assess the extent of bone and soft tissue involvement. Plain radiographs are not sufficient for evaluation. Beware that penetrating trauma to the midface may involve injury to the brain and major vascular structures. Therefore, a CT scan of the head and diagnostic angiography should also be considered.
- Cerebrospinal fluid (CSF) leak (primarily type II and type III fractures)
- Epistaxis is commonly associated with Le Fort type II and III fractures
