Compartment Syndrome
Published (updated: ).
Introduction

Acute compartment syndrome occurs when there is increased pressure within a closed osteofascial compartment, resulting in impaired local circulation. Acute compartment syndrome is considered a surgical emergency since, without proper treatment, it can lead to ischemia and eventually necrosis. Generally, acute compartment syndrome is considered a clinical diagnosis. However, intracompartmental pressure (ICP) > 30 mmHg can be used as a threshold to aid in diagnosis. However, a single normal ICP reading does not exclude acute compartment syndrome.
Fascia is a thin, inelastic sheet of connective tissue that surrounds muscle compartments and limits the capacity for rapid expansion. In the leg, there are four muscle compartments: anterior, lateral, deep posterior, and superficial posterior. The anterior compartment of the leg is the most common location for compartment syndrome. This compartment contains the extensor muscles of the toes, the tibialis anterior muscle, the deep peroneal nerve, and the tibial artery.
Other locations in which acute compartment syndrome is seen include the forearm, thigh, buttock, shoulder, hand, and foot. It can also be seen in the abdomen, but more commonly, it presents in the limbs.
Significant attention should be paid to patients with open fractures. Recent retrospective studies indicate that skin laceration would not relieve the pressure inside the muscle compartments. Therefore, acute compartment syndrome is still predictable.
Etiology
Acute compartment syndrome can occur with any condition that restricts the intracompartmental space or increases the fluid volume in the intracompartmental space. Acute compartment syndrome can occur without any precipitating trauma but typically occurs after a long bone fracture, with tibial fractures being the most common cause of the condition, followed by distal radius fractures. Seventy-five percent of cases of acute compartment syndrome are associated with fractures. After fractures, the most common cause of acute compartment syndrome is soft tissue injuries. Other causes of acute compartment syndrome include burns, vascular injuries, crush injuries, drug overdoses, reperfusion injuries, thrombosis, bleeding disorders, infections, improperly placed casts or splints, tight circumferential bandages, penetrating trauma, intense athletic activity, and poor positioning during surgery.
In children, supracondylar fractures of the humerus and both ulnar and radial forearm fractures are associated with compartment syndrome.
Epidemiology
The incidence of acute compartment syndrome is estimated to be 7.3 per 100,000 in males and 0.7 per 100,000 in females, with the majority of cases occurring after trauma. Tibial shaft fracture is the most common cause of acute compartment syndrome, is associated with a 1 to 10 percent incidence of acute compartment syndrome.
Acute compartment syndrome occurs more commonly in males younger than 35, which may be due to a larger relative intracompartmental muscle mass and increased likelihood of being involved in high-energy trauma.
Patients with bleeding diathesis, such as hemophilia, are at greater risk for acute compartment syndrome. Cases of acute compartment syndrome have been reported without acute precipitating trauma in pediatric leukemia.
Patients who develop acute compartment syndrome without any fracture are at a higher risk of developing complications and delayed treatment.
Pathophysiology

Acute compartment syndrome occurs due to decreased intracompartmental space or increased intracompartmental fluid volume because the surrounding fascia is inherently non-compliant. As the compartment pressure increases, hemodynamics are impaired. There is normally an equilibrium between venous outflow and arterial inflow. When there is an increase in compartmental pressure, there is a reduction in venous outflow. This causes venous pressure and, thus, venous capillary pressure to increase. If the intracompartmental pressure becomes higher than arterial pressure, a decrease in arterial inflow will also occur. The reduction of venous outflow and arterial inflow result in decreased oxygenation of tissues causing ischemia. If the deficit of oxygenation becomes high enough, irreversible necrosis may occur.
The normal pressure within a compartment is less than 10 mmHg. If the intracompartmental pressure reaches 30 mmHg or greater, acute compartment syndrome is present. However, a single normal ICP reading does not exclude acute compartment syndrome. ICP should be monitored serially or continuously.
History and Physical
Acute compartment syndrome typically occurs within a few hours of inciting trauma. However, it can present up to 48 hours after. The earliest objective physical finding is the tense, or ”wood-like” feeling of the involved compartment. Pain is typically severe, out of proportion to the injury. Early on, pain may only be present with passive stretching. However, this symptom may be absent in advanced acute compartment syndrome. In the initial stages, pain may be characterized as a burning sensation or as a deep ache of the involved compartment. Paresthesia, hypoesthesia, or poorly localized deep muscular pain may also be present.
Classically, the presentation of acute compartment syndrome has been remembered by “The Five P’s”: pain, pulselessness, paresthesia, paralysis, and pallor. However, aside from paresthesia, which may occur earlier in the course of the condition, these are typically late findings. Beware that the presence or absence of a palpable arterial pulse may not accurately indicate relative tissue pressure or predict the risk for compartment syndrome. In some patients, a pulse is still present, even in a severely compromised extremity.
Physical exam should focus on the neurovascular territory of the involved compartment:
- Observe skin for lesions, swelling, or color change
- Palpate over the compartment, observing temperature, tension, tenderness
- Check pulses
- Evaluate two-point discrimination and sensation
- Evaluate motor function
Although the clinical features discussed above can help identify compartment syndrome, they have limited sensitivity and specificity. Other factors, such as compartment pressures, can help make the diagnosis.
Due to the potential for rapid progression of compartment syndrome, clinicians should perform serial exams.
Evaluation
Acute compartment syndrome is a clinical diagnosis and needs prompt treatment. However, the following are done to evaluate further and to confirm the diagnosis.
- Radiographs should be obtained if a fracture is suspected
- Measurement of intracompartmental pressure is not required but can aid in diagnosis if uncertainty exists. Compartment pressures are often measured with a manometer, a device that detects intracompartmental pressure by measuring the resistance that is present when a saline solution is injected into the compartment. Another method employs a slit catheter, whereby a catheter is placed within the compartment, and the pressure is measured with an arterial line transducer. The slit catheter method is more accurate and allows for continuous monitoring. Its use is also recommended to measure all the surrounding compartments.
- The normal pressure within the compartment is between 0 mmHg to 8 mmHg.
- An intra-compartmental pressure greater than 30 mmHg indicates compartment syndrome and a need for fasciotomy.
- When intra-compartmental pressure increases to within 10 mmHg to 30 mmHg of the patient’s diastolic blood pressure, this indicates inadequate perfusion and relative ischemia of the involved extremity.
- The perfusion pressure of a compartment, also known as the compartment delta pressure, is defined as the difference between the diastolic blood pressure and the intra-compartmental pressure:
- delta pressure = diastolic pressure – measured intracompartmental pressure
- clinicians often utilize delta pressure less than or equal to 30 mmHg as indicative of the need for fasciotomy.
- Ultrasound with Doppler can be used to look for occlusion or thrombus.
- Elevations in creatine phosphokinase (CPK) may suggest muscle breakdown from ischemia, damage, or rhabdomyolysis.
- If rhabdomyolysis is being considered, renal function tests, urine myoglobin, and urinalysis should be done.
- If rhabdomyolysis is diagnosed, a chemistry panel is needed.
- Preoperative studies should, at a minimum, include a complete blood count and coagulation studies.
Treatment / Management
Acute compartment syndrome is an emergency condition. Less time should be spent on confirmation of the diagnosis, as delayed treatment may result in loss of limb.
- Immediate surgical consult
- Provide supplemental oxygen.
- Remove any restrictive casts, dressings, or bandages to relieve pressure.
- Keep the extremity at the level of the heart to prevent hypo-perfusion.
- Prevent hypotension and provide blood pressure support in patients with hypotension.
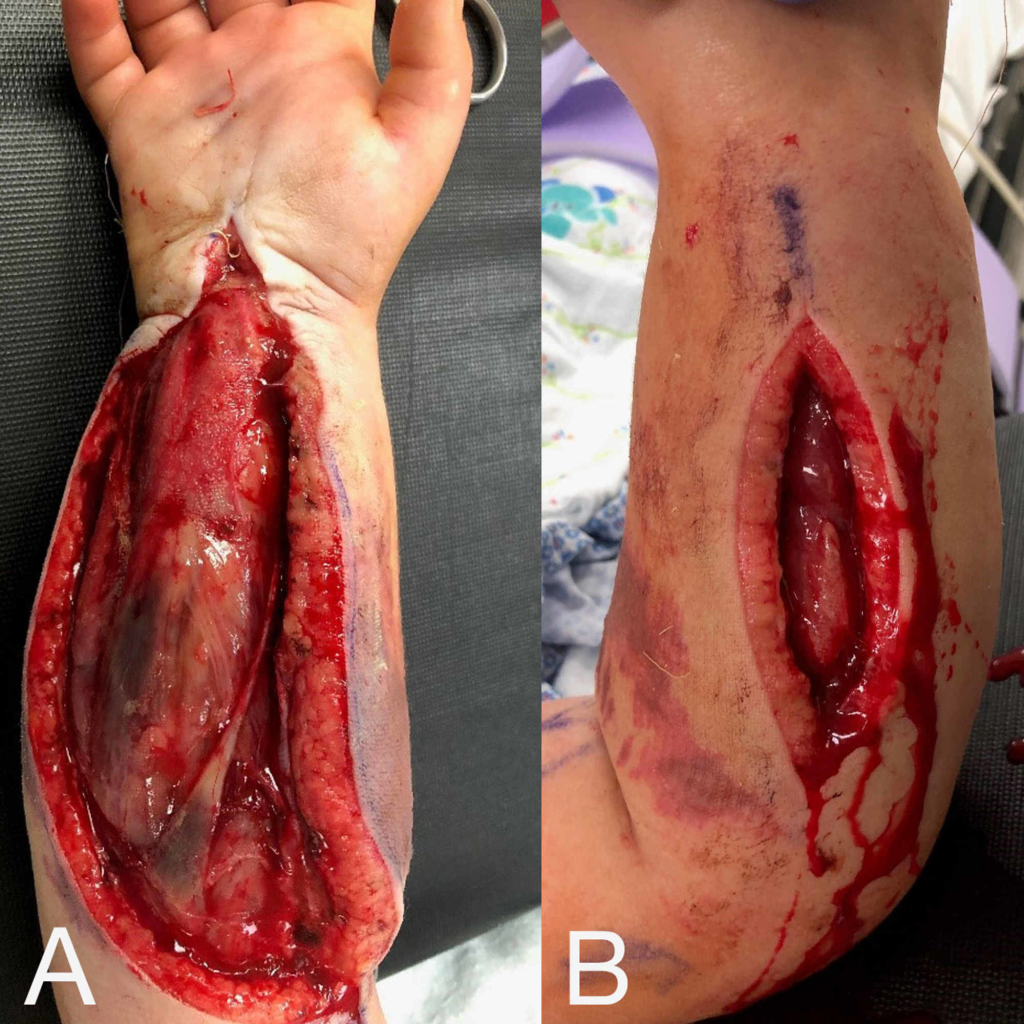
- If ICP is greater than or equal to 30 mmHg or delta pressure is less than or equal to 30 mmHg, fasciotomy should be done.
