Rib Fractures
Published (updated: ).
When enough force is placed on the rib, the rib will fracture. Most isolated rib fractures can be managed expectantly. However, certain patterns of rib fractures are associated with higher morbidity and mortality and will need further evaluation for other underlying injuries and emergent treatment.
Introduction
Rib fractures occur when a significant enough force directed at the rib causes a break. There are a total of 12 pairs of ribs in the thoracic region. The first seven ribs attach anteriorly to the sternum and posteriorly to the spinal column. Rib numbers 8 through 10 attach similarly but connect to the costal cartilage of the sternum anteriorly. Ribs 11 and 12 have the name of “floating” ribs as they only attach posteriorly but do not attach anteriorly. Underneath each rib lies the intercostal nerve, artery, and veins which supply to blood supply and innervation. The ribs function to protect the underlying organs and structures of the thoracic cavity. Any rib fracture should warrant a thorough evaluation of any concomitant injury, including lungs, heart, kidney, spleen, liver, and neuro-vasculature.
Etiology
Rib fractures can be traumatic or atraumatic. Most rib fractures are due to direct penetrating or blunt trauma to the chest. Ribs 1 through 3 are the hardest to break and signify a significant degree of trauma if fractured. Ribs 4 through 10 are typically the most vulnerable while ribs 11 through 12 are more mobile and therefore more difficult to break. In the elderly, falls are a common etiology of rib fractures and are associated with higher mortality and morbidity than younger patients. Rib fractures may also be pathologic as a result of cancer metastasis from other organs. Through repetitive stress and microtrauma, athletes can develop rib fractures with chronic use. Spontaneous rib fractures can also occur due to severe cough and are more likely to occur in those with osteoporosis or underlying lung disease. Because children tend to have more elastic ribs than adults do, children are less likely to sustain rib fractures. Therefore, children with rib fractures is a sign of significant trauma and should warrant an investigation of possible child abuse.
Epidemiology
The incidence and prevalence of rib fractures depend on the injury and the severity of the trauma. Children are less likely to sustain rib fractures than adults due to their more elastic ribs. The elderly tend to be more prone to rib fractures than younger individuals, with higher mortality and morbidity.
Pathophysiology
Rib fractures can occur from either direct penetrating or blunt trauma. Athletes can also develop specific patterns of stress fractures depending on their sport. The most feared complication of rib fractures is the flail chest where three or more rib fractures at two points on the involved ribs, creating a floating rib segment and causes this segment to move paradoxically with the rest of the chest wall. The mortality rate of flail chest is between 10% to 15%.
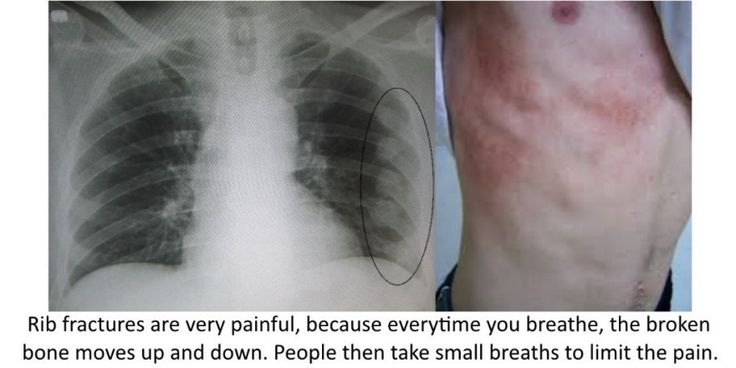
Most isolated rib fractures are diagnosable through a clinical exam. Typically, patients will provide a history of recent blunt or penetrating thoracic trauma and pain at that site. They may also exhibit decreased ability to perform full inspiration due to pain. The physical exam may reveal chest wall bruising, along with bony tenderness to palpation or crepitus. Any vital sign abnormalities such as hypoxia, tachypnea, or significant respiratory distress should undergo further evaluation of other possible injuries such as pneumothorax, hemothorax, cardiac and pulmonary contusions. Lower rib segment injuries should undergo assessment for kidney, liver, and spleen. Any patient with paradoxical chest wall movement or suspicion for multiple rib fractures should be evaluated for flail chest and managed accordingly.
History and Physical
Rib fractures can be diagnosed clinically based upon history and physical exam without imaging. Dedicated rib x-ray series are typically not necessary due to the benign clinical course of isolated rib fractures. If there is suspicion for multiple rib fractures or significant trauma with underlying organ damage, imaging can be the next step.
Prognosis
Depending on the severity of the trauma sustained and degree of pain, rib fractures may be managed either outpatient or inpatient. Isolated rib fractures tend to heal well and do not need any further interventions beyond pain control, rest, and ice. Multiple rib fractures, displaced rib fractures, or those with underlying concomitant injuries may require inpatient monitoring for respiratory failure or surgical correction. Elderly individuals with rib fractures tend to have a higher mortality rate than younger individuals and may require closer monitoring.
Complications
The most severe complications related to rib fractures are the flail chest and damage to the underlying structures. Solid organ injuries associated with rib fractures include liver injuries and splenic injuries. Typically, the higher the rib fracture is within the thoracic cage, the more likely it is to cause a liver or splenic injury. Particular attention needs to be paid for the patient’s respiratory status, as rib fractures may cause the patients to go on and develop acute respiratory failure due to poor respiratory efforts and may need mechanical ventilation and surgical stabilization.
