Aortic Disruption
Published (updated: ).
Introduction
In the United States, trauma remains the leading cause of death in those less than 44 years of age, and for those older than 45, trauma is one of the top five causes of death. Of all injuries sustained in trauma, the aortic injury is one of the most time-sensitive, life-threatening conditions, second only to head injury as a cause of death. The morbidity and mortality associated with traumatic aortic injury are about 30% within the first 24 hours. Some predisposing factors for traumatic aortic injury include; penetrating chest injuries, deceleration injuries, and blunt chest trauma. There are no clinical findings specific for aortic injury. However, hypotension, external evidence of trauma, and altered mental status are common. Many patients with complete transection of the thoracic aorta die before arriving at the emergency department (ED). Those who survive arrival in the ED may have small tears or partial-thickness tears of the aortic wall with a pseudo-aneurysm formation. The survival of patients after traumatic aortic injury depends on a clinician’s high index of suspicion, rapid diagnosis, and prompt management.
Etiology
Blunt force trauma is more common. This involves rapid deceleration mechanisms such as motor vehicle accidents or falls from great heights. Aortic trauma can also be caused by penetrating traumas, such as stab injury and firearm injury.
Epidemiology
It is the second most common cause of death in patients with blunt force trauma (head trauma is the most common). Over 80% of those with aortic injury die at the scene. Up to 15% of all deaths following motor vehicle collisions are due to injury to the thoracic aorta.
Pathophysiology
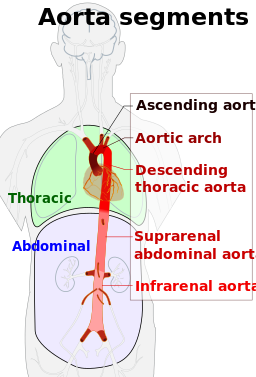
The aorta has some fixed regions, particularly the relatively fixed aortic arch (to the thoracic inlet by the brachiocephalic vessels). The remaining portions of the aorta are relatively free. Ascending and descending aorta are relatively mobile except at specific points. These can result in an unequal distribution of shear forces on the relatively fixed arch and mobile ascending and descending aorta and stress at the site of attachment of the aorta, particularly the aortic root and the aortic isthmus.
Major mechanisms involved in aortic trauma injuries are as follows:
- Rapid acceleration and deceleration. Significant deceleration occurs in head-on collisions or lateral impact. The greatest risk involves frontal or side impacts.
- Significant falls, greater than 4 meters can also result in aortic trauma. These involve the thoracic aorta. In this case, significant physical forces can result in; blunt force compression of chest wall contents (particularly the aorta against the spinal column and tearing of the aorta). In addition, this type of trauma may cause the vertebral column, sternum, first rib, and clavicle to compress the aorta in the region of the isthmus.
- Twisting against fixation points – usually, twisting of the aorta at the ligamentum arteriosum just distal to the left subclavian artery can also result in aortic trauma.
- Seatbelt injuries: This involves the abdominal aorta. Although the abdominal aorta is relatively rarely injured in blunt trauma, severe trauma may disrupt the abdominal aorta.
- Other high-risk mechanisms involved in blunt aortic trauma such as the ejection of an unrestrained passenger from the vehicle, and injuries resulting in death at the scene of the accident.
- Mechanism of injury: rupture of the adventitia. This can cause lethal internal hemorrhage.
Type of injury:
- Intimal tear: This leads to disruption of the media and can cause a false lumen.
- Mediastinal hematoma: Since traumatic aortic injury differs from spontaneous aortic injury with respect to the involvement of multiple layers of the aorta, mediastinal hematoma usually develops secondary to trauma.
- Transection of the aorta: Complete rupture of the aorta, including the adventitial layer and periadventitial connective tissue, results in immediate exsanguination.
Beware that delayed adventitial rupture may occur during hospitalization.
History and Physical
History
There are no clinical findings specific for aortic injury. However, hypotension, external evidence of trauma, and altered mental status are common.
The symptoms may include the following:
- Chest pain: Usually retro-sternal, or intra-scapular pain
- Difficulty breathing or swallowing
- Dysphagia, stridor, or a hoarse voice, may occur due to pressure from a mediastinal hematoma.
Be aware that symptoms may not reliably predict aortic injury.
Physical Examination
- Usually, no clinical signs of traumatic aortic injury are present in patients with aortic injury
- Steering wheel marks or seatbelt signs may be present.
- A discrepancy may exist between the blood pressures in each arm. Upper-extremity hypertension
- Femoral pulses may be diminished or absent
- Pseudo-coarctation: Increased blood pressure in upper extremities and lower blood pressure in the lower extremities
- A new heart murmur not previously present
