Getting Ventilation Right With Capnometry
Published .
End-tidal carbon dioxide (ETCO2) is the level of carbon dioxide that is released at the end of an exhaled breath. ETCO2 levels reflect the adequacy with which carbon dioxide (CO2) is carried in the blood back to the lungs and exhaled. Available evidence has established that ETCO2 measurement can provide an indication of cardiac output and pulmonary blood flow. Non-invasive methods for ETCO2 measurement include capnometry and capnography. Capnometry provides a numerical value for ETCO2. In contrast, capnography delivers a more comprehensive measurement that is displayed in both graphical (waveform) and numerical form. For this reason, capnography is currently the most widely recommended method for monitoring ETCO2.
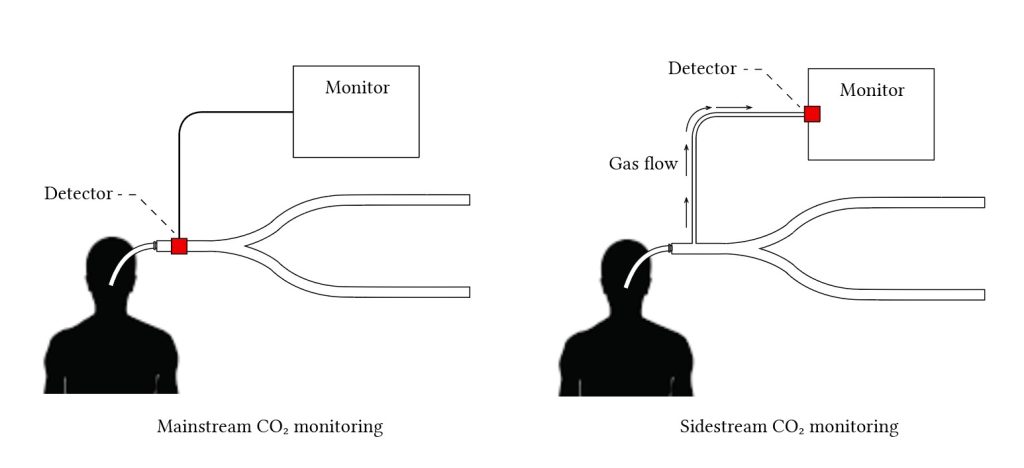
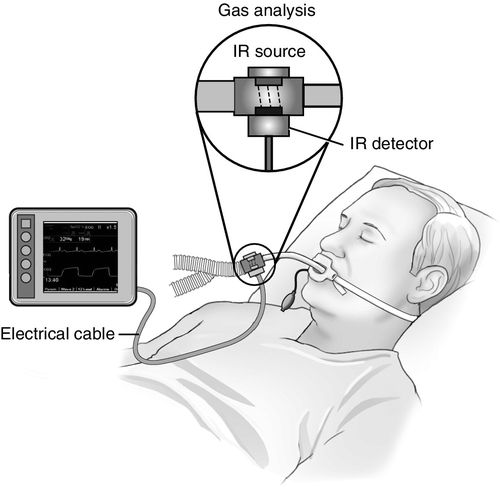
Capnography devices are configured as either sidestream or mainstream. In a sidestream configuration, the CO2 sensor is located in the monitoring device, which is at a distance from the patient. The exhaled CO2 is diverted from the airway into the device via a sampling tube of six to eight feet in length, which is attached to the breathing circuit fitted to the patient. In the case of a mainstream configuration, the CO2 sensor and a sampling cell are integrated into a small device that connects directly at the airway, between the breathing circuit and endotracheal tube (ETT). Sidestream devices can monitor both intubated and non-intubated patients, while mainstream devices are most often limited to intubated patients. Sidestream measurement has been the most common type of ETCO2 measurement modality in Canadian facilities, even as a number of new, innovative, and ultraportable mainstream capnography devices are becoming available. Whether sidestream or mainstream, capnography devices are available as hand-held portable devices or as a module or component integrated into other medical equipment, such as defibrillators, anesthesiology machines, and patient-monitoring systems.
By using capnography, a patient’s ventilation status is monitored in real time. Health care providers are able to identify potential breathing complications (such as airway obstruction, hyperventilation, hypoventilation, or apnea) and respond accordingly with a change in clinical management (for example, providing supplemental oxygen or reassessing the patient). Detecting issues at an early stage prompts timely intervention at the onset of an adverse respiratory event, which can help avoid deterioration to a more critical, or fatal, point. A 2011 audit of major airway-management complications in the United Kingdom (UK) estimated that 82% of events resulting in death or brain injury in the intensive care unit (ICU) likely ensued from failure to use capnography in relevant cases. The same audit concluded that half of the deaths that occurred in UK emergency departments could have been avoided had capnography been correctly used and interpreted. However, if capnography is used or interpreted incorrectly, the falsely high or falsely low readings may potentially lead to unnecessary patient interventions. Capnography may also capture an otherwise self-resolving incident of respiratory depression, which might also lead to unnecessary interventions.
ETCO2 monitoring using capnography devices has application across several hospital and pre-hospital settings and, depending on the clinical area, the technology is at various stages of adoption. Anesthesiologists have been using capnography for decades to monitor ETCO2 in patients receiving general anesthesia. The monitoring devices help to prevent or reduce adverse events, such as otherwise undetected respiratory depression and hypoxia.
More recently, advances in both technology and scientific understanding of the value of ETCO2 monitoring, particularly capnography, have expanded its use beyond anesthesiology. Capnography is also used to monitor the effectiveness of cardiopulmonary resuscitation (CPR) in patients with cardiac arrest; for continuous monitoring of patients in the emergency room and ICU; during ambulatory transport; and to confirm the correct placement of an ETT. The American Heart Association’s Advanced Cardiovascular Life Support guidelines, for example, now carry recommendations for the use of quantitative waveform capnography during CPR. Emerging evidence and expert recommendations also suggest that capnography may be valuable in the early post-operative period. Post-operative patients, especially those with a known history of obstructive sleep apnea or who are receiving high doses of opioids for the management of pain, are at an increased risk of adverse respiratory events. Some experts believe that monitoring ventilation with ETCO2 measurement, in addition to pulse oximetry, could improve patient safety and post-operative clinical outcomes.
