Heat Injuries
Published (updated: ).
The disorders of hyperthermia, also known as heat-related injury or illness, exist on a continuum, which is marked by dysregulation of the body’s thermoregulatory capacity. This condition can vary both in presentation and in severity, from benign conditions, including heat cramps and heat edema, to life-threatening hyperthermia, also known as heatstroke. It is essential to be able to identify and manage these conditions appropriately as moderate hyperthermia can progress to life-threatening heatstroke. As such, including these injuries in medical decision-making, prompt identification, and appropriate treatment is important. This article will also review the epidemiology, including at-risk populations, red-flag features of patient presentations, treatment options and strategies, and preventative techniques, which all play a significant role in decreasing the morbidity, mortality, and healthcare costs associated with these injuries.
Etiology
Humans are homeotherms, which means we are organisms capable of maintaining our body’s temperature in a specific range. While baseline body temperature is between 36.5 to 37.5°C (97.7 to 99.5°F), the body has mechanisms to address temperatures between approximately 35 to 41°C (95.0 to 105.8°F), after which it can no longer self-regulate and compensate for external thermal loads. The body’s core temperature is the sum of metabolic heat production, mechanical work, and heat exchange with the environment. A balance between internal and external variables (e.g., levels of metabolically active hormones, external temperature and humidity, and the amount of environmental convection) affects the body to cause either a net gain or a net loss of temperature. Heat exchange with the environment occurs through evaporative, convective, conductive, and radiative loss. As external temperature and humidity rise, radiation and conduction become ineffective, and evaporative dissipation of heat is the primary means by which the body can cool itself.
This process is monitored and affected through sensory receptors. Thermoreceptors found in the skin, organs, and spinal cord relay information via afferent nerve fibers to the preoptic area of the hypothalamus. This response causes autonomic and behavioral changes that help correct body temperature back to baseline. Physiologic changes include vasodilation of blood vessels, with the majority of flow occurring primarily in the peripheral arteriovenous anastomoses (AVA). The highest concentration of AVAs are present in the glabrous tissues, including the hands, feet, and face, and, as such, are important areas to address during treatment with rapid cooling.
Other physiologic changes include an increased rate of sweat production via sympathetic cholinergic receptors and decreased metabolism leading to decreased internal heat production. It also elicits behavioral modifications, but these are under voluntary control. Examples of these include the desire to seek shade or shelter, use air-conditioning or forced convection with fans, and loosen clothing or shed insulating layers. As these are under voluntary control, individuals are at an increased risk for heat illness when they ignore these impulses either consciously or subconsciously. An example of this is athletes who push themselves to train in hot conditions or in elderly residents who may not possess access to air-conditioning units during heat waves or the means to evacuate from an unsafe environment.
Comorbidities, mental status changes, and medications may also play a role in limiting a person’s response to exposure to a hot environment.
Epidemiology
Heat illness is a common issue experienced worldwide. The National Oceanic and Atmospheric Administration have found it to be the number one cause of weather-related fatalities year after year. This data also has support from data published by the Centers for Disease Control. In the United States between 2001 and 2010, a network of 20 states had had a total of 28,133 hospitalizations for heat illness, with a majority of cases occurring in males and persons 65 years or older. Of the participating states, the majority of hospitalizations occurred in the midwest and southern states, which have consistent exposure to higher index temperatures throughout the year. Support for this concept exists from correlations found in that data set between the number of hospitalizations and the monthly maximum temperature/heat index. These findings were not just limited to the United States but also found in many other countries worldwide. There are also gender differences, with these conditions occurring more often in males. This data may be due to a disproportional number of males that engage in manual labor, including work outdoors in construction or in mine shafts, which combine physical exertion in a hot environment with limited airflow.
Risk factors for the development of heat-related illness include:
- High temperatures and humidity
- Heatwave (greater-than-or-equal to three days of temperature more than 32.2°C (90.0°F))
- Age (older and young patients)
- Obesity
- Concurrent infection
- Hydration status
- Alcohol consumption
- Drugs including but not limited to: diuretics, anticholinergics, beta- or calcium-channel blockers, antihistamines, amphetamines
- Comorbid medical conditions including diabetes mellitus, infections, skin disorders, sickle cell trait, and cardiovascular disease
In addition to older patients who have many of the risk factors presented above, specific population groups that are susceptible to heat-related injuries include adolescents and athletes. Although heat injury appears to be more significant in the elderly due to decreased health reserves, it also frequently occurs in adolescents and teenagers during the summer months, which may be due to increased participation in activities outside, including in sports. Athletes, in general, are at considerable risk of heat illness and heat stroke, which research shows the latter of these has to be the third-highest cause of mortality in this population. The risk for all groups of people increases in these environments due largely to a large volume of sweat loss accompanied by clinically significant sodium and chloride loss leading to dehydration.
Younger children are at particular risk for developing heat-related injury due to multiple factors, including:
- An increased surface area to body mass ratio
- Decreased blood volume
- Immature thermoregulatory mechanisms
- A higher set point for sweat-inducing temperature compensation in addition to less sweat volume
- Slower ability to acclimatize to hotter environments
Modifiable risk factors for the development of heat illness include obese body habitus, alcohol use, medication use, illicit stimulant drug use, hydration status, and avoidance of exertion in hot and humid environments.
History and Physical
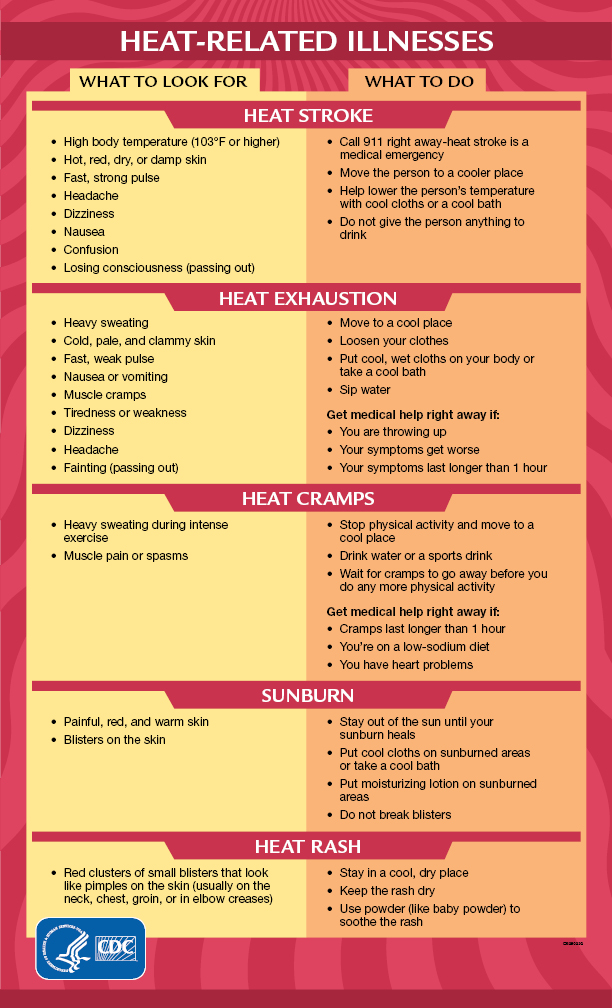
Obtaining an accurate history from the patient, family, bystanders, or first responders is of pivotal importance as this can help determine what the patient was doing when symptoms started and in what environment they were found. Symptoms of heat illness vary depending on which form of heat injury has occurred. The following are a list of various heat-related injuries:
- Heat edema: swelling and possible discomfort in the distal extremities due to vasodilation and gravity-dependent pooling of fluids. An example of this would be an older individual who has recently arrived at an environment hotter than previously accustomed to with dependent swelling in the extremities after one to two days. Individuals may complain that gloves or shoes feel tight due to this acral swelling.
- Heat rash (also known as miliaria or prickly heat): caused by obstruction of eccrine sweat glands during exposure to hot climates. The use of restrictive clothing or occlusive objects like bandages may exacerbate heat rash.
- Heat cramps: involuntary spasmodic contractions of large muscle groups as opposed to an isolated muscle spasm/cramp that can also occur during or after exertion. This condition is due to a relative deficiency of sodium, potassium, chloride, or magnesium. Other symptoms may include nausea, vomiting, fatigue, weakness, sweating, and tachycardia.
- There has previously been a distinction between muscle cramping due to heat exposure and cramping caused by exertion, also known as exercise-associated muscle cramps (EAMCs). The reason behind this is because research has shown that exertion-related cramping is not necessarily related to elevated body temperature, it does not occur with passive heating at rest, and it can be present during exercise in cool, temperature-controlled environments. Regardless, the treatment, as described below, is the same for both cramping conditions.
- Heat syncope: temporary, self-limited dizziness, weakness, or loss of consciousness during prolonged standing or positional changes in a hot environment, including physical activity. The thinking is that it is due to a combination of dehydration, pooling of blood in the venous system, decreased cardiac filling, and low blood pressure, which leads to decreased cerebral blood flow.
- Heat stress or heat exhaustion: symptoms usually include any combination of nausea, vomiting, dizziness, light-headedness, irritability, headache, thirst, weakness, excessive sweating, muscle cramps, and decreased urine output in the setting of high body temperatures. External temperatures may be more moderate if associated with intense physical exertion. Survey-based data has shown that some of the most common symptoms are headache, exhaustion, or a combination of symptoms. Body temperature is not usually elevated at or above 40.5°C [105°F]. Heat exhaustion can progress to life-threatening heatstroke if immediate interventions, including removal from the hot environment, are not carried out.
- Heat injury: presents with similar symptomatology as heat exhaustion and includes organ injury or dysfunction (cardiac, renal, hepatic, gut, or musculoskeletal injury).
Central nervous system involvement with symptoms or signs that may include seizures, gait abnormalities, delirium, coma, etc., in the setting of elevated temperature cause concern for heatstroke, as described elsewhere.
Evaluation
History and physical examination may be all that is necessary to make the diagnosis, and it is not uncommon that testing, including lab work, is normal. If a patient’s presentation is concerning for heat stress, heat injury, or heatstroke, a core temperature should be obtained with rectal thermometry if clinically possible. Laboratory tests are not typically necessary unless there is a concern for electrolyte imbalance, significant dehydration, or organ injury, or to investigate other diagnoses. Because of the risk for critical cardiovascular collapse found with progression to heatstroke, further testing may be warranted depending on the severity of clinical presentation.
Treatment / Management
In general, the initial treatment of heat illness involves stopping the activity and moving the individual to a cool environment, as all of these conditions will benefit from cooling. Supportive care is the recommended strategy for the more benign conditions described above, including heat edema, syncope, rash, and cramps. For more serious presentations, including heat exhaustion, resuscitation should occur as typical to address concerns that may exist for airway, respiratory, or cardiovascular compromise and, if present, may warrant emergent transportation to a higher level of care. Otherwise, oral rehydration with water or an electrolyte-containing drink can commence on-site. Studies have previously shown that oral and IV rehydration are equivalent for the treatment of heat illness. Care should be taken not to overhydrate patients as some may be sensitive to significant volume status changes, including patients with a decreased cardiac function. Specific strategies are as follows:
- Heat edema: elevation of the affected limbs and compression garments can help with dependent swelling. There is no role for diuretic medications for heat edema.
- Heat rash/miliaria: a staple of treatment includes the avoidance of tight-fitting clothing. Symptoms are treatable with topical lotions like calamine or steroids of mid-potency like triamcinolone 0.1% cream, which will also help with inflammation. If there is any concern for bacterial superinfection, as may be seen in the pustulosa form or the development of impetigo, topical antibiotics should be considered with selection towards those with adequate staphylococcal coverage like mupirocin.
- Heat cramps: The patient should cease physical activity and initiate oral rehydration. Rest and massage or passive stretching of the muscle groups have also been demonstrated to be helpful. Additional treatment with medications, including diazepam, magnesium, or calcium, is not effective.
- Heat syncope: the treatment also includes replacement of fluid losses with a preference towards oral rehydration over parenteral rehydration. Supine positioning with leg elevation above the level of the heart can also be helpful. Orthostatic vital sign measurements can be considered an adjunct to monitor for adequate replacement in addition to the resolution of symptoms during positional changes.
- Heat stress, exhaustion, and injury: more aggressive measures at cooling should occur, including lukewarm water sprayed over the skin with forced air conduction to promote evaporation and consideration towards parenteral rehydration if the patient cannot tolerate oral rehydration due to symptoms or degree of injury. Further, the correction of electrolyte and divalent disturbances may also require intervention.
The differential diagnosis for these presentations includes:
Differential Diagnosis
- Infectious etiologies like tetanus, sepsis, or meningoencephalitis are similar concerning alterations in mental status, body temperature setpoints, and focal neurologic changes that may mimic heat-related injury.
- Primary metabolic abnormalities, including endocrine dysfunction like thyroid storm or diabetic ketoacidosis
- Neurologic insults, including stroke or primary seizure disorder
- Toxicologic ingestions including anticholinergic toxidrome, neuroleptic malignant syndrome, serotonin syndrome, and withdrawal symptoms
Specific heat illnesses can also have symptoms that mimic other syndromes. For example, heat edema should not be mistaken for swelling caused by other medical conditions, including hypervolemia from congestive heart failure or liver dysfunction or a deep vein thrombosis of the extremity. Heat syncope should not be confused for syncope of other etiology, including cardiogenic or with different pathologies that lead to a transient change in consciousness (e.g., pulmonary embolism, rupture of an ectopic pregnancy, aortic dissection, or some environmental gas exposures).
Prognosis
The prognosis for the more benign heat illnesses described above is excellent. They are self-limited and resolve with removal from the hot environment and supportive care with rehydration and electrolyte replacement.
Complications
The minor heat illnesses are benign and self-limited with no ongoing complications. For the more moderate heat illnesses, including heat exhaustion/stress and heat injury, complications are exacerbated by the patient’s age, comorbidities, the presence of organ injury, or if severe electrolyte disturbances have occurred. These patients may benefit from admission to a tertiary care center for further stabilization before discharge. Predictive factors for hospitalization include the age of equal to or greater than 65 years, the level of temperature elevation, alterations in mental status, and elevations of creatinine from baseline.
