Symptoms Associated With Injuries To Various Parts Of The Brain
Published (updated: ).
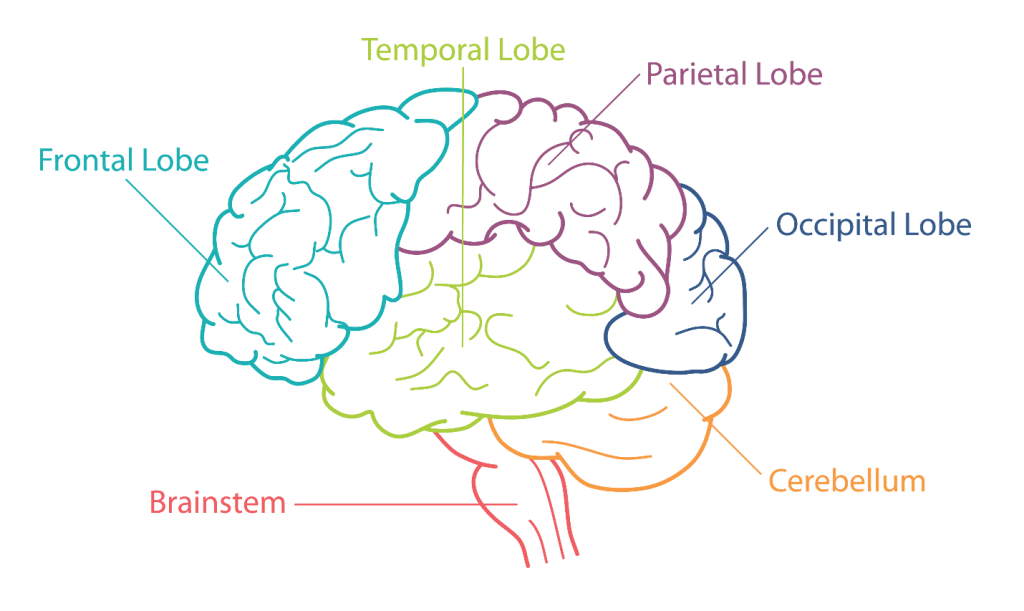
Cerebral cortex injuries lead to cognitive, emotional, and sensory deficits
The cerebral cortex is the outer layer that lies on top of the cerebrum. The cerebrum is the largest area of the brain and divides the brain into two sides called hemispheres which are attached by a bundle of nerve fibers called the corpus callosum. When the cerebral cortex is injured the patient is most likely to experience cognitive, sensory, or emotional deficits.
Brainstem injuries result in posturing, bradycardia, and strange respiratory patterns
The brainstem is a lower part of the brain connected to the spinal cord. The brainstem is responsible for regulating most of the body’s automatic functions that are responsible for life; these include breathing and controlling heart rate. When the brain stem is damaged, the patient may experience bradycardia. Bradycardia from brain stem trauma is due to pressure applied to the vagus nerve. Abnormal respiratory patterns are also seen with brain stem injuries. Patient’s with injury to the brain stem may display decerebrate posturing. Decerebrate posturing is an abnormal body posture that involves the arms and legs being held straight out; it has been pointed downward, and the head and neck arched backwards Patients with brain stem injuries also experience seizures.
Increased intracranial pressure symptoms get worse with more pressure
Bleeding or swelling in the brain can lead to damage to other parts of the brain that were not immediately affected by the trauma. Given the fact that the brain only provides a certain amount of space for the brain and blood vessels, any additional bleeding or swelling would increase the pressure inside the skull. Increased intracranial pressure is associated with the following symptoms:
- Decrease level of consciousness
- Increased blood pressure and slowing pulse rate
- The people’s will remain reactive
- Cheyne Stokes respirations – Cheyne Stokes breathing is a type of abnormal breathing. It’s characterized by a gradual increase in breathing, and then a decrease. This pattern is followed by a period of apnea where breathing temporarily stops. The cycle then repeats itself.
- Patients are typically (at least initially) responsive to painful stimuli
- Good outcomes are possible for when identified and the patient transported to a capable hospital.
Injuries to the pons result in central neurogenic hyperventilation
The middle of the brainstem is referred to as the pons. As a part of the brain stem it links the brain to the spinal cord. The pons handle unconscious processes and jobs, such as sleep-wake cycle and breathing. It also contains several junction points for nerves that control muscles and carry information from senses in the head and face. The pons is the primary respiratory center and is located underneath the medulla. Its main function is to control the rate or speed of involuntary respiration. Medics should suspect an injury to the pons when treating an unresponsive head injury patient with nonreactive or sluggish pupils, wide pulse pressure, and bradycardia. Patients with injuries to the pons will often exhibit central neurogenic hyperventilation. The decerebrate posturing is also common among patients with injuries to the pons.
Medulla injuries lead to unequal pupils and ataxic respirations
The medulla is the bottom of part of the brain connecting the spinal cord through the foramen magnum. The foramen magnum is an opening at the bottom of the skull. Just above the medulla is the pons which is below the central structures of the brain. The medulla also separates the nerves that control muscle movement, which are on the left side, and the nerves that control certain sensations like touch temperature in pain, which are on the right side. Medics should suspect an injury to the medulla or lower brain stem when they find unequal pupils (anisocoria). Patients with injuries to the lower brain stem or medulla often display ataxic respirations. Ataxic respirations are an abnormal pattern of breathing characterized by complete irregularity of breathing, with the irregular pauses and increasing periods of apnea. As the breathing pattern deteriorates it merges with agonal respiration. The patient with a medulla injury will respond placidly to painful stimuli. Patients with injuries to the lower brain stem or medulla are often hypertensive and bradycardic.
Assessment of patients with brain injuries
The initial observation made by medics is the patient’s level of responsiveness. Medics should always assess the airway of patients who are not alert. Patients who are not alert could be verbally responsive, painfully responsive, or unresponsive. After the patient has been loaded in the ambulance the medics should consider calculating a Glasgow Coma Scale (GCS). A GCS greater than 13 suggest a mild head injury while a GCS between 8 and 12 suggest a moderate head injury. Severe head injuries are considered when the patient has a GCS of less than 8. The patient’s vital signs can also point to a head injury even though not all head injuries produce hypertension. Assessment of pupils can also be helpful in determining the nature of the brain injury. The SAMPLE history will reveal clues about the patients level of consciousness immediately after the injury occurred. Improving oxygenation it’s always a goal for medics when treating a brain injury. The brain injury patient may breathe normally or display any number of alternate respiratory patterns.
Management of brain injuries
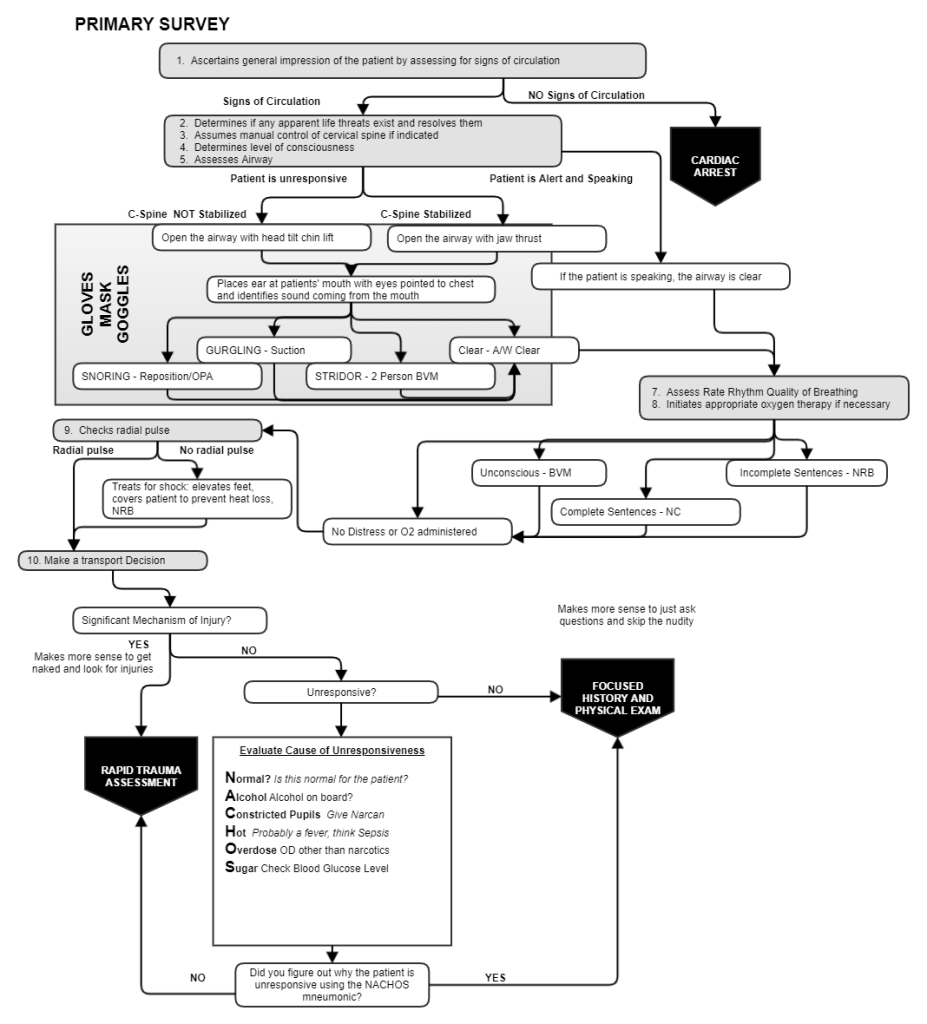
Initial management of the patient is always guided by the primary survey. During the primary survey the medics should consider the possibility of a cervical spine fracture based on the mechanism of injury. Patients wearing helmets may need them removed in order to manage airway and breathing. If possible, the helmet would be better left on the patient’s head (as long as the airway can be assessed and maintained). It is important that medics know how to open, assess and manage a patient’s airway while cervical spine precautions are being maintained. Manually stabilizing the cervical spine, then opening the airway with a jaw thrust, then ventilating with a bag valve mask cannot be performed by 1 rescuer but must be performed by 2. Opening the patient’s airway with a head tilt chin lift may result in worsening of a patient cervical spine fracture. It is recommended that patients with potential brain injuries be positioned with her head elevated at a 30° angle from their body.
