Abnormal Breathing From Head Injuries
Published .
There are multiple types of normal and abnormal respiration. They include apnea, eupnea, orthopnea, dyspnea, hyperpnea, hyperventilation, hypoventilation, tachypnea, Kussmaul respiration, Cheyne-Stokes respiration, sighing respiration, Biot respiration, apneustic breathing, central neurogenic hyperventilation, and central neurogenic hypoventilation. Each pattern is clinically important and useful in evaluating patients.
Function
Evaluating respiratory patterns assists the clinician in understanding the patient’s current physiologic status. Abnormal breathing patterns suggest the possibility of an underlying injury or metabolic derangements. Early recognition of abnormal respiratory patterns can aid the clinician in early intervention to prevent further deterioration of the patient’s condition.
Issues of Concern
Breathing is controlled centrally in the brainstem. It receives input from central and peripheral chemoreceptors as well as voluntary control from the cerebrum. The brainstem also receives input from the chemoreceptors and adjusts the rate and tidal volume based on pH and PaCO2.
The regular cycle of breathing originates in the medulla. The medullary respiratory center has several widely dispersed groups of neurons referred to as the dorsal and ventral respiratory groups. There do not appear to be separate inspiratory and expiratory centers.
Bilateral dorsal respiratory groups (DRG) control the rhythm of breathing by producing inspiratory impulses. Neurons from this center send impulses to the motor neurons of the diaphragm and the external intercostal muscles. These nerves also extend to the ventral respiratory groups (VRG). Input from the airways, lungs, joint proprioceptors, and peripheral chemoreceptors via the vagus and glossopharyngeal nerves modify the breathing pattern.
The ventral respiratory groups (VRG) are also bilateral collections of inspiratory and expiratory neurons in the medulla and are active in exercise and stress. These neurons send impulses to the diaphragm and external intercostals. They also stimulate the abdominal muscles and internal intercostals via neurons in the caudal area.
The interaction between the DRG and VRG produces an impulse, the inspiratory ramp signal. It starts low and gradual, then increases to produce a smooth inspiratory effort.
The pons contains two respiratory areas referred to as the pneumotaxic and apneustic centers. The pneumotaxic center has an inhibitory effect on the medulla. In effect, its stimulation causes the end of the inspiratory effort and therefore controls the inspiratory time. Weak signals from the pneumotaxic center increase inspiratory time, causing an increase in tidal volume. The apneustic center stimulates the inspiratory neurons in the medulla and inhibits the expiratory neurons. Overstimulation of this area produces long, gasping inspirations that are interrupted inadequately by occasional expirations. This pattern is called apneustic breathing.
Clinical Significance
The types of clinically relevant normal and abnormal respiration patterns include the following:
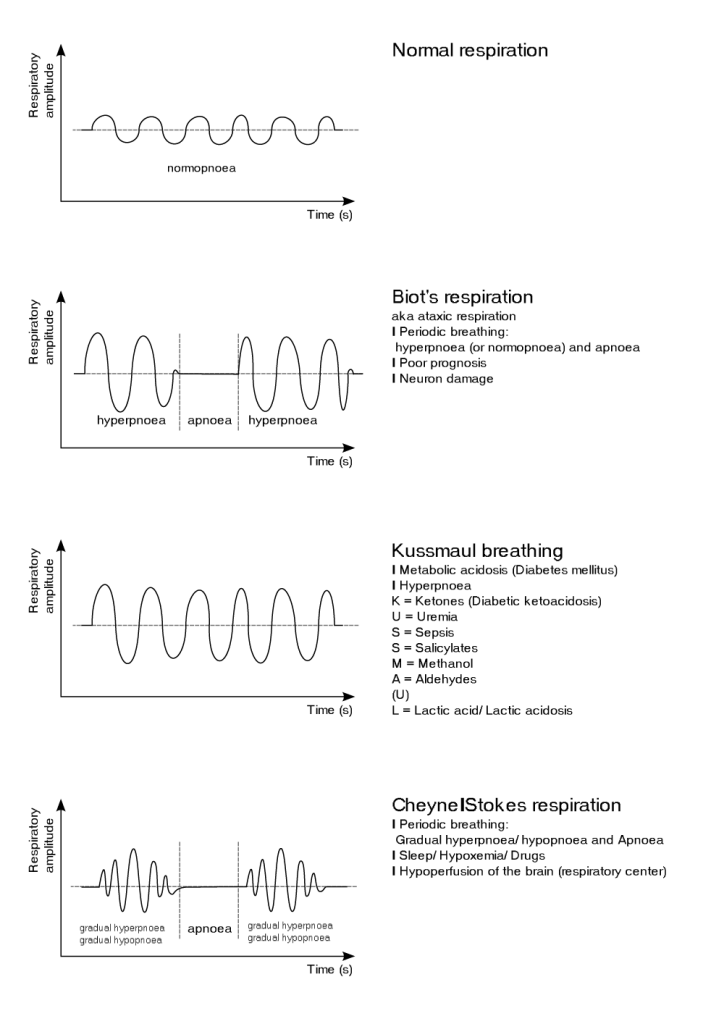
- Eupnea is normal breathing.
- Sighing is an involuntary inspiration that is 1.5 to 2 times greater than normal tidal volume. Sighing breathing is observed in subjects suffering from anxiety with no observed organic pathology.
- Dyspnea is the subjective sensation of difficulty breathing.
- Paroxysmal nocturnal dyspnea is described as attacks of severe shortness of breath that wake the patient from sleep. They have to sit up to catch their breath. Most commonly, this is a symptom of heart failure.
- Orthopnea also is seen in heart failure. Patients are unable to breathe comfortably, lying flat. They must be in a sitting or propped up to breathe without difficulty.
- Cheyne-Stokes is a pattern of crescendo-decrescendo respirations followed by a period of apnea. This pattern of breathing was first described by John Cheyne, a British Physician, and William Stokes, an Irish Physician. It is well described in patients with heart failure. Usually observed while asleep and is the result of disordered central control of breathing. Its presence has implications for outcome in that cardiac resynchronization therapy improves outcomes in patients with Cheyne-Stokes respirations.
- Bradypnea is a respiratory rate that is lower than normal for age.
- Tachypnea is a respiratory rate that is greater than the normal for age.
- Hyperpnea in increased volume with or without an increased rate of breathing. Blood gasses are normal.
- Agonal breathing is characterized by slow, very shallow irregular respirations that result from anoxic brain injury. This will often progress to apnea depending on the underlying cause.
- Apnea is the absence of breathing. This signals a life-threatening situation in which the patient will quickly succumb unless rescue breathing is instituted immediately.
- Hyperventilation is over-ventilation above that needed for the body’s CO2 elimination. This results in a decrease in PaCO2 and respiratory alkalosis. Hyperventilation can be driven by chemoreceptor stimulation due to metabolic acidosis.
- Hypoventilation is under-ventilation below that needed for the body’s CO2 elimination. It is inadequate to maintain a normal PaCO2.
- Kussmaul respirations were originally observed and described by Dr. Adolf Kussmaul in 1874. He made his observation in patients with diabetes mellitus who were comatose and in the late stages of diabetic ketoacidosis. As classically described, Kussmaul respirations are a deep, sighing respiratory pattern. Dr. Kussmaul actually described it as “air hunger.” This is probably the most important of the abnormal respiratory patterns.
- Kussmaul respiratory pattern occurs due to increased tidal volume with or without an increased respiratory rate. It is a form of hyperventilation. It results from stimulation of the respiratory center in the brain stem by low serum pH. The effect is the lowering of the partial pressure of carbon dioxide in the alveoli, thereby compensating for metabolic acidosis. Initially, in acidosis, the respiratory pattern is rapid and shallow, but as the acidosis progresses, the inspirations become deeper. It is only in the later stages that true Kussmaul respirations are seen. Kussmaul respirations can be seen with any disorder that causes significant acidosis. Toxic ingestions, particularly alcohols, are another common cause of Kussmaul respirations. Salicylate toxicity is also a cause. Kussmaul was also classically described in patients with uremia. It can also be seen in any disorder that results in lactic or ketoacidosis.
- Acidosis results from the abnormal accumulation of ketones, lactate, urate, or exogenous acid in the blood. A fall in pH significant enough to induce Kussmaul respiration is a sign of decompensation. As described by Dr. Kussmaul, this respiratory pattern is a perimortem event. Failure to recognize this respiratory pattern can result in delayed recognition and treatment of the underlying cause. Such delays can result in increased morbidity and even mortality for the patient.
- The Biot respiratory pattern was first described by Camille Biot, a French physician, in 1876. He made his observations while studying the pattern of breathing described by John Cheyne and William Stokes. Biot respiratory pattern is characterized by regular deep respirations interspersed with periods of apnea. It is caused by damage to the pons due to stroke, trauma, or uncal herniation. As the insult to the pons progresses, the pattern becomes irregular. At this point, the pattern deteriorates to ataxic breathing. Biot respiratory pattern can also be induced by opiate intoxication.
- Apneustic breathing is another abnormal breathing pattern. It results from injury to the upper pons by a stroke or trauma. It is characterized by regular deep inspirations with an inspiratory pause followed by inadequate expiration. This respiratory pattern is often associated with severe brain injury and carries a poor prognosis. Apneustic breathing can be temporarily induced by ketamine. Central neurogenic hyperventilation is persistent hyperventilation typically caused by head trauma, severe brain hypoxia, or lack of cerebral perfusion. It is usually due to the midbrain and upper pons damage. Central neurogenic hypoventilation occurs when the medulla respiratory centers are not responding to appropriate stimuli. Central neurogenic hypoventilation may occur with head trauma, cerebral hypoxia, and narcotic suppression.
Breathing patterns associated with brain injury may not be observed due to mechanical ventilation and sedation. There is a complex interplay in cases that result in brainstem injury. The autoregulation of cerebral blood flow is affected by CO2 levels in the blood. As CO2 increased, cerebral vessels will dilate, and as they decrease, the cerebral vessels will constrict. In traumatic brain injury (TBI), the brain swells and cannot expand due to the fixed volume of the intact skull. Raised intracranial pressure can overcome perfusion pressure causing further anoxia and injury leading to brain death and/or herniation. Although hyperventilation can lower PaCO2, causing vasoconstriction and reduce swelling/ICP, it should be avoided. The effect is short-lived. In TBI, both hyperventilation and hypoventilation must be avoided. ICP is treated pharmacologically, surgically, and with medically induced coma.
