Management Of Orthopedic Trauma
Published .
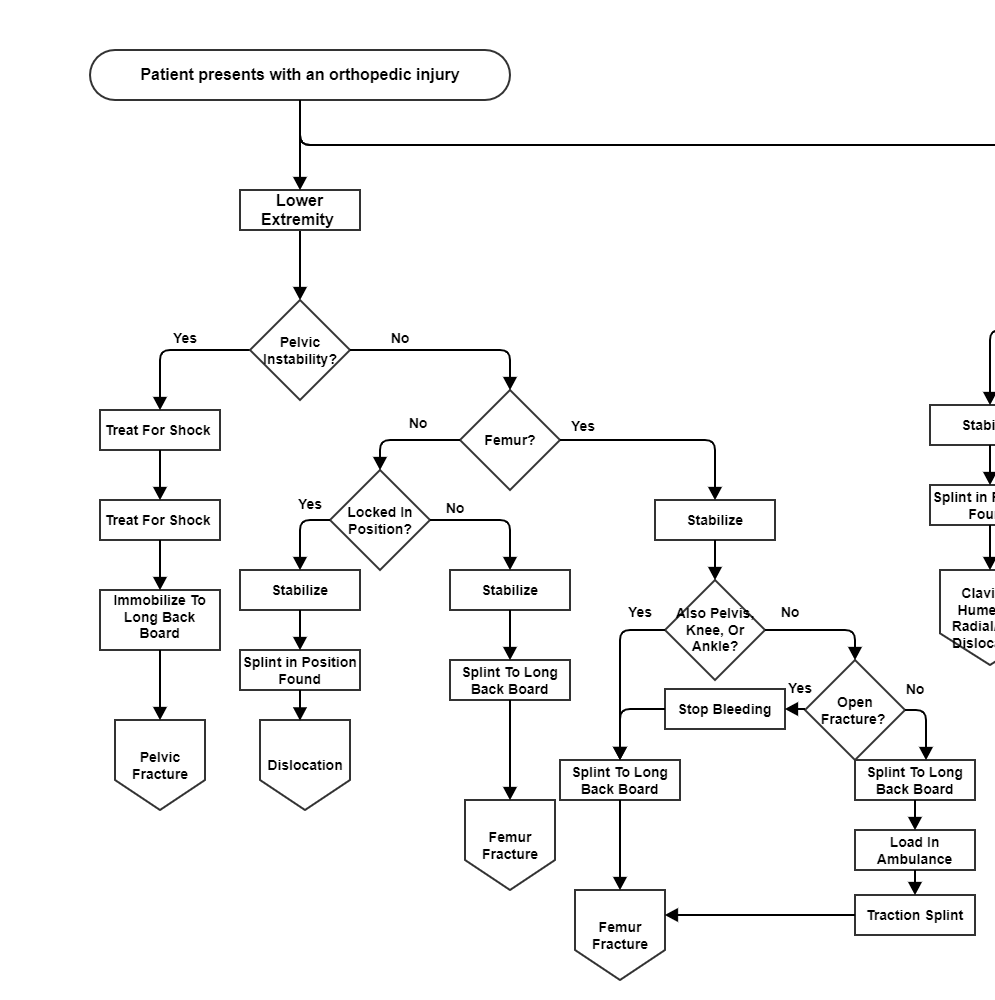
Pelvic fractures need to be stabilized prior to movement, however this is not always possible to even identify these injuries. Further, utilizing MAST trousers as recommended is impossible in Georgia as ambulances no longer carry them. On the market are various pelvic straps that can be used for this purpose. Despite all of these options, there actually seems to be no consensus for the movement of a patient with a pelvic fracture. This fact should underscore the importance of handling patients with care.
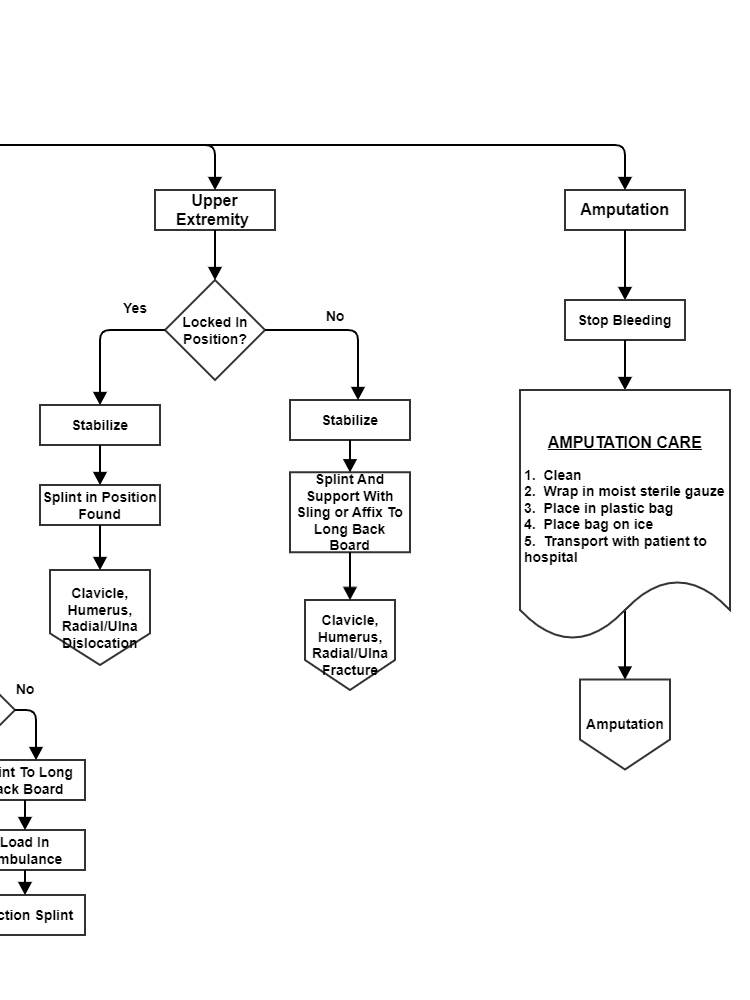
All fractures require immediate stabilization. Stabilization is where a rescuer holds the broken extremity and keeps it from moving. The rescuer is now a splint, and remains a splint until a mechanical splint can be devised. Georgiaemsacademy primary teaches 2 types of splints, a padded board with sling and swathe for upper extremities and a long back board for lower extremities. Lower extremity fractures carry the added complexity of the patient not being able to walk. A long back board serves as an excellent splint and an even better litter.
Georgiaemsacademy has always taught to splint femur fractures to the long backboard, then address the possibility of a utilizing a traction splint. Too much time is taken on scene measuring and placing a traction splint on a patient prior to movement on scene. The use of a traction splint requires assessing the possibility of a pelvic, knee, tibia/fibula, or ankle fracture. These decisions would be better made miles away from the scene in the back of the ambulance.
Splinting is not just for fractures, but also dislocations. If a dislocation or other deformity is locked in a position where the medics can splint with a sling and swathe or long backboard, then that is what they should do. Else, a medic will need to stabilize the extremity all the way to the ambulance and then all the way to the hospital.
