More About Long Bone Fractures
Published .
Various Mechanisms Of Injury
Skeletal fractures can occur from both direct impact and indirect loading and are caused when the load, whether compression, tension or shear, in a localised part of the bone exceeds the strength of the bone. The severity of the fracture will depend on the energy associated with the impact or loading, and the direction and location of the load in the bone. There are several methods for classifying different types of fracture, and recording the severity of the fracture, which are dependent on the treatment and long-term prognosis. There are four main fracture mechanisms: –
- Direct impact (Flat plate blunt object injuries)
- Direct Penetration (gun shot / sharp object injuries)
- Indirect Loading (inertia and crushing injuries)
- Repetitive loading (fatigue)
There is often direct and indirect impact resulting from a significant mechanism of injury. For instance, let’s say the patient is injured in motor vehicle accident. The direct impact of the dashboard breaks the patients tibia. Secondly, indirect loading produced by inertia of the occupants own mass sometimes will result in a femur fracture following knee impact into a seat back in unidirectional seating, or attempting to brace while falling.
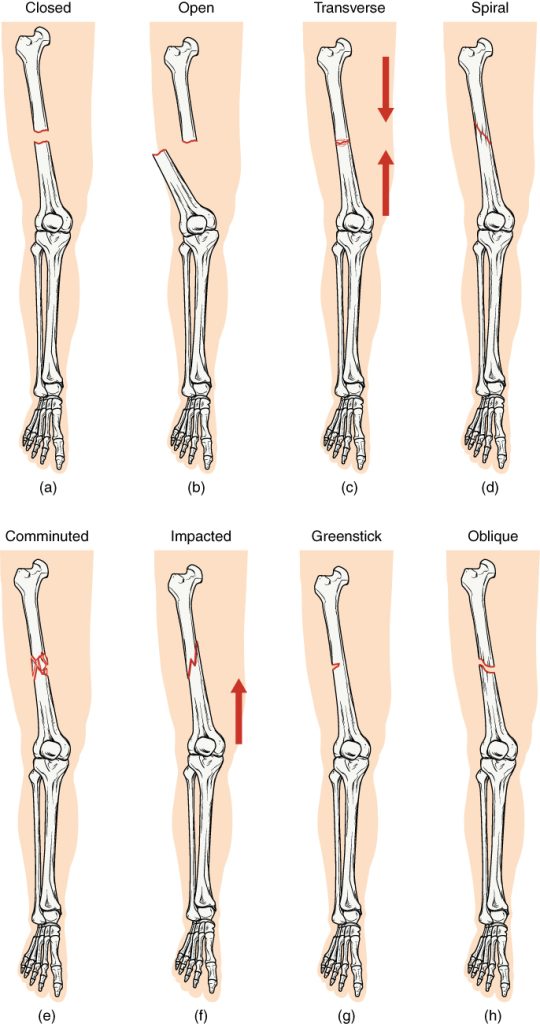
| Type of fracture | Description |
|---|---|
| Transverse | Occurs straight across the long axis of the bone |
| Oblique | Occurs at an angle that is not 90 degrees |
| Spiral | Bone segments are pulled apart as a result of a twisting motion |
| Comminuted | Several breaks result in many small pieces between two large segments |
| Impacted | One fragment is driven into the other, usually as a result of compression |
| Greenstick | A partial fracture in which only one side of the bone is broken |
| Open (or compound) | A fracture in which at least one end of the broken bone tears through the skin; carries a high risk of infection |
| Closed (or simple) | A fracture in which the skin remains intact |
The severity of fracture is classified by the type and number of fracture surfaces, which is dependent on the energy of the impact. Non-comminuted or single surface fractures are produced by low energy impacts, typical falling and bracing injuries, while comminuted or multiple surface fractures a rise from high energy impacts such as pedestrian to vehicle impacts. The higher the energy, the higher the number of fracture surfaces, with high velocity bullets literally shattering the bone. In the rail vehicle environment the majority of fractures will be from low energy indirect bracing injuries to medium energy impacts, such as the direct impact of a flailing arm on a rigid blunt object.
In low energy impacts the fracture can occur with no displacement along the fracture surface with a very high probability of a fast recovery, with no surgical intervention or long-term disabilities. With medium and high energy impacts with both non-comminuted and comminuted fractures, displacement along the fracture surface(s) is inevitable requiring moving of the bones to ensure correct setting. With comminuted fractures surgical intervention with the using of pins and plates to correctly locate the parts of the fractured bone is essential, which increases the time of recovery and probability of long-term disability.
Compounding the severity of the actual bone fracture is the amount of soft tissue damage associated with it. Low energy fractures would be associated with only minor lacerations (cuts) and contusions (bruising) with the bone unexposed, and this is classified as a closed fracture. With medium and high energy impacts the fractured portions of the bone are often forced through the muscle and skin and exposed, and so is classified as an open fracture. With the increasing amount of bone exposed there is a corresponding increase in the probability of contamination of the wound, with consequences for increased time of recovery and long-term disfigurement and disability.
The fractures occur both at diaphysis part of the bone, the hard ‘cortical’ bone, away from the articular or joint surfaces, or at the epiphysis directly through the articular surface or immediately behind it. Fractures in the Epiphysis tend to be more complicated with much poorer prognosis due to the damage to the load bearing surface and bone growth areas, leading to long-term joint problems and growth abnormalities. These are more difficult to classify in terms of loading mechanisms, but could be more attributed to axial or angled indirect compression loading of the joint from low to high energies. Pylon or longitudinal fracture of the lower tibia is a good example caused by high axial loading of the ankle produced in falling vertically on to a rigid surface (parachuting), or by footwell intrusion in vehicle frontal accidents.
Soft Tissue Damage
There are two major mechanisms, which cause non-skeletal or soft tissue injuries.
- Direct impact injuries producing lacerations (cuts) and contusions (bruises) to the actual skin penetrating into the soft tissue underneath
- Indirect loading injuries, produced especially at joints, where excessive motion causes tearing of muscles, tendons and ligaments, or joint dislocation
Indirect Load Joint And Soft Tissue Injuries
High loads and excessive joint displacements and rotations are produced either from direct impacts, knee dislocation from impact with lower seat backs, or by occupants bracing themselves to avoid impacts, shoulder dislocations during stumbling.
The occupants mobility and is often associated with joint cartilage and ligament damage, which has long-term consequences especially in complex joints such as the wrist and ankle. However, these injuries are very difficult to predict and, except for full joint dislocations, may not be apparent immediately after the incident.
