Abdominal Injuries
Published .
Closed Injuries
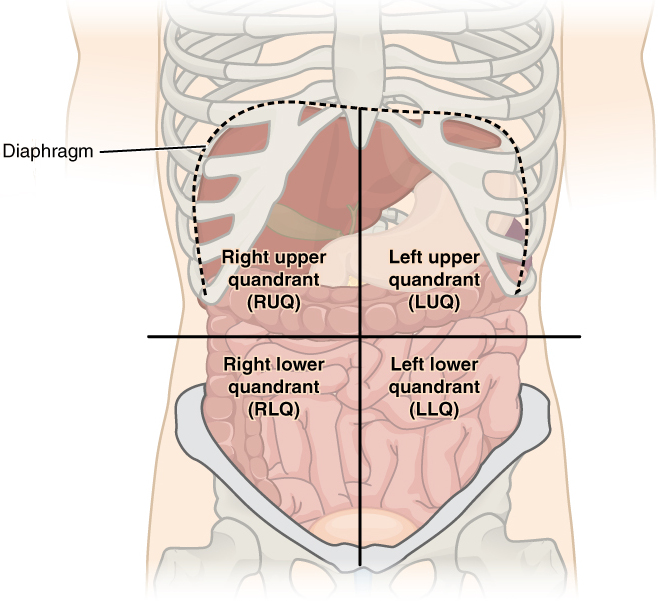
Most abdominal injuries are the result of blunt force trauma. Trying to figure out what organs were injured or bleeding can be challenging, however, the location of pain, tenderness, or discoloration (bruising) can provide clues as to the exact nature of the patient’s injuries.
Aside from making an educated guess based on the location of the patient’s pain, the medics could appreciate the mechanism of injury. The most common mechanism of injury that results in occult (hidden) abdominal injuries is blunt force trauma. The following are common blunt force trauma mechanism of injuries:
- Compression – Crushing force applied to abdomen
- Deceleration – Deceleration injury can be defined as an impact injury to a body within or upon a rapidly moving object caused by the forces exerted when the object comes to a complete stop. Deceleration injury generally takes place in high-speed vehicles when they abruptly stop or when the vehicles slow down, or when the occupants are propelled from the vehicle while it is moving. The majority of deceleration experiments have been conducted in connection with air travel, where the acceleration factor is typically much greater than in land vehicles.
- Motor Vehicle Accident (MVA) – MVA’s often present the possibility of the patient’s body impacting with the inside of the vehicle or even getting thrown out of the car. Being strapped in doesn’t guarantee the patient will be injury free. Deceleration injuries are common in motor vehicle accidents, especially at higher speeds.
- Falls – The patient falls and impacts the ground causing injury. Further injuries are related to deceleration
- Assault
- Blast Injuries – Explosions can produce unique patterns of injury seldom seen outside combat. When they do occur, they have the potential to inflict multi-system life-threatening injuries on many persons simultaneously. The injury patterns following such events are a product of the composition and amount of the materials involved, the surrounding environment, delivery method (if a bomb), the distance between the victim and the blast, and any intervening protective barriers or environmental hazards. Because explosions are relatively infrequent, blast-related injuries can present unique triage, diagnostic, and management challenges to providers of emergency care.
Open Injuries
Penetrations are easy to see and require no imagination to understand the severity of the injury. The penetration can range from a small hole to a massive gaping wound. Penetrating abdominal trauma is most commonly caused by stabbing or gunshot wounds. The most commonly injured regions are the small bowel, large bowel, liver, and intra-abdominal vasculature.
Penetrating abdominal trauma is seen in many countries. The most common cause is a stab or gunshot. The most common organs injured are the small bowel (50%), large bowel (40%), liver (30%), and intra-abdominal vascular (25%). When the injury is sustained at close range, there is more kinetic energy than those injuries sustained from a distance. Even though most gunshot wounds typically have a linear projection, high-energy wounds are associated with unpredictable injuries. There may also be secondary missile injuries from bone or bullet fragments. Stab wounds that penetrate the abdominal wall are difficult to assess. Occult injuries can be missed, resulting in delayed complications that can add to the morbidity.
Penetrating trauma occurs when a foreign object pierces the skin and enters the body creating a wound. In blunt or non-penetrating trauma the skin is not necessarily broken. In penetrating trauma, the object remains in the tissue or passes through the tissues and exits the body. An injury in which an object enters the body and passes through is called a perforating injury. Perforating trauma is associated with an entrance wound and an exit wound.
Penetrating trauma suggests the object does not pass through. Penetrating trauma can be caused by violence and may result from:
- Fragments of a broken bone
- Gunshots
- Knife wounds
Penetrating trauma often causes damage to internal organs resulting in shock and infection. The severity depends on the body organs involved, the characteristics of the object, and the amount of energy transmitted.
Puncture and penetration are similar.
- A puncture does not have an exit wound. It is generally due to something sharp or pointed
- This type of trauma is seen in a stabbing or when stepping on a nail.
As a projectile passes through tissue, it decelerates and transfers kinetic energy to the tissue. Increased velocity causes more damage than mass. Kinetic energy increases with the square of the velocity.
The space left by tissue that is destroyed by the penetrating object forms a cavity, and this is called permanent cavitation. In addition to the damage to the tissues they contact, medium- and high-velocity projectiles result in a secondary cavitation injury as the object enters the body, it creates a pressure wave forcing tissue out of the way, creating a cavity. The tissues move back into place, eliminating the cavity, but the cavitation has already done considerable damage.
The characteristics of the damaged tissue determine the severity of the injury: the denser the tissue, the greater the amount of energy transmitted to it.
Penetrating abdominal trauma is due to stabbings, ballistic injuries, and industrial accidents. These injuries may be life-threatening because abdominal organs bleed profusely. If the pancreas is injured, further injury occurs from autodigestion. Injuries of the liver often present in shock because the liver tissue has a large blood supply. The intestines are at risk of perforation with concomitant fecal matter complicating penetration.
Penetrating abdominal trauma may cause hypovolemic shock and peritonitis. Penetration may diminish bowel sounds due to bleeding, infection, and irritation, and injuries to arteries may cause bruits. Percussion reveals hyperresonance or dullness suggesting blood. The abdomen may be distended or tender indicating surgery is needed.
The mortality rate from penetrating abdominal trauma depends on the organ involved, time to therapy, and how many other organs are involved. The literature reveals mortality rates from 0-100%. The lowest mortality is in patients who sustain just a superficial injury to the abdominal wall but if the injury penetrated the peritoneum and is associated with hypotension, acidosis, and hypothermia, the mortality rates are more than 50%. The mortality is greatest in those who suffer a concomitant vascular injury of the abdominal vessels. When the patient is brought promptly to a trauma center, a 5% mortality rate can be expected. The majority of deaths occur within the first 24 hours of injury. Risk factors that predict mortality include female gender, the presence of shock on arrival, delay in treatment, and associated head injury. Firearms are usually associated with much higher morbidity and mortality compared to knife wounds.
