Chest Wall Related Injuries
Published .
Trauma is the third leading cause of death in all age groups after cardiovascular diseases and cancer. Although trauma-related injuries can occur in many parts of body, one out of four trauma patients die due to thoracic injury or its complications. Chest trauma remains a serious problem as high-speed vehicle accidents increase. Thoracic trauma occurs in approximately 60% of patients with polytrauma and has a mortality of 20%–25%.
Trauma can be divided into two types: penetrating and blunt. Penetrating injuries such as penetrating, cutting and firearm injuries are disruptive to tissue integrity. Blunt injuries can cause damage to organs and structures under the tissue without disrupting the integrity of the tissue. Falling from height, traffic accidents and occupational accidents are main mechanisms of blunt injuries. Considering that 70% of all chest traumas constitute blunt injuries, the importance of blunt injuries is understood. In addition, blunt chest trauma accounts for 15% of all trauma cases in the world. The mortality rate is hard to evaluate as the causes of death in blunt chest trauma may be due to pulmonary and non pulmonary complications.
In addition, the age of the patient is important when evaluating a blunt chest trauma. While a trauma in the pediatric age group may not cause a chest wall injury due to bone elasticity, it may lead to serious complications and even death in the elderly population. It also can be interpreted that even if there is a serious trauma in the pediatric age group, the number of fractures may not be high due to bone elasticity, but in the elderly population the number of bone fractures may be high even in a slight trauma.
Blunt traumas are defined as injuries that organs and structures were injured without disrupting tissue integrity. Blunt traumas can also be classified according to their mechanisms. The mechanism of blunt trauma can be listed as motor vehicle accident, occupational accident and fall. It is important to know the mechanism of blunt injury for a rapid diagnosis and treatment, because there are specific injuries caused by different mechanisms, and the mechanism of injury is an independent factor of mortality.
Most of the blunt thoracic trauma are caused by motor vehicle accidents (includes pedestrian accidents) and falls from height. Motor vehicle accidents are the most common cause of severe thorax trauma. The best example of acceleration-deceleration damage is a motor vehicle accident. The most common condition is the sudden and high-speed deceleration of the anterior thorax, resulting in injury to the vascular structures, bones, soft tissues and organs. At the same time, the presence of steering wheel deformity caused by the driver hitting the steering wheel increases thoracic injuries, complications and mortality. Thoracic compression is usually caused by crush, occupational accident and fall from height.
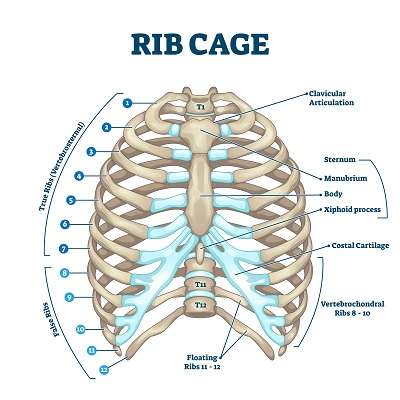
The most common injury in blunt thoracic trauma is chest wall injury, which also includes rib fractures. When bone fractures are mentioned, not only rib fractures but also clavicle and sternum fractures should be considered. Isolated rib fractures are not fatal. However, the rib fractures are usually accompanied by additional damage such as damage of pleura and lung tissue, pneumothorax, hemothorax, pulmonary contusion and parenchymal laceration, etc. The affacted rib usually fractured from the point of blunt impact or from the posterolateral bend, which is the most vulnerable part.
The first two ribs are strongly attached to the musculoskelatal system, making them more difficult to break. Thus, the first rib fractures have a high mortality rate of 36%. Because it can cause injury to the subclavian vessels and brachial plexus. Fracture of the first ribs is a high risk indicator for tracheobronchial, vascular, cardiac and pulmonary injuries.
Middle zone ribs 4 to 9 are heavily exposed to blunt trauma. Fractures of these midzone ribs are often associated with injuries such as pulmonary contusion, laceration, hemothorax and pneumothorax. Rib fractures can cause various injuries and pulmonary complications as well as intraabdominal organ injuries. Although the last two ribs are more mobile and less fractured, fractures may result in liver, spleen and kidney injuries.
Contusion of chest wall tissue is another common problem in blunt trauma. These minor incidents do not cause serious problems and therefore they are not widely reported. However, contusion and abrasion of chest wall tissue can cause bleeding by injuring vessels in the skin, subcutaneous tissue, and muscles. In severe trauma patients, this type of bleeding can be persistent and cause problems. Contusion of chest wall tissue should be kept in mind, although it is often ignored in the medical literature.
Flail chest is a condition in which three or more contiguous ribs are broken at least in two parts. Basically, flail chest occurs when a segment of the chest wall is disconnected from the rest of chest wall. As the flail segment loses its continuity, the chest wall paradoxically moves in different directions during inspiration and expiration. In the inspiration, the ribs move outward while the flail chest moves inward; in the expiration, the opposite occurs. This is called paradoxical motion.
Flail chest is often caused by blunt trauma to the thorax, such as direct blows, falls from height, and car accidents. Flail chest is usually not alone, but with additional injuries resulting in shock and blood loss. A trauma strong enough to form a flail segment may also cause parenchymal contusion. As a result of pulmonary contusion, the breathing mechanism is impaired and edema and even necrosis may occur with pulmonary tissue bleeding. The presence of pulmonary contusion is highly predictive of morbidity. Flail chest is also closely associated with injuries such as hemothorax and pneumothorax.
Paradoxical movement makes breathing difficult and can cause respiratory failure. Paradoxical motion may not be seen because the breathing is shallow due to pain, therefore, the diagnosis can be difficult. However, flail chest can be diagnosed with careful inspection, palpation, percussion and auscultation For this reason, flail chest patients should be examined by removing the clothes in order to perform a careful physical examination. Although patients may have a good clinical appearance, they should be kept under close observation since their condition may deteriorate. Paradoxical respiratory movement is typical for the diagnosis. Patients may also have severe chest pain and signs of respiratory distress, such as tachypnea.
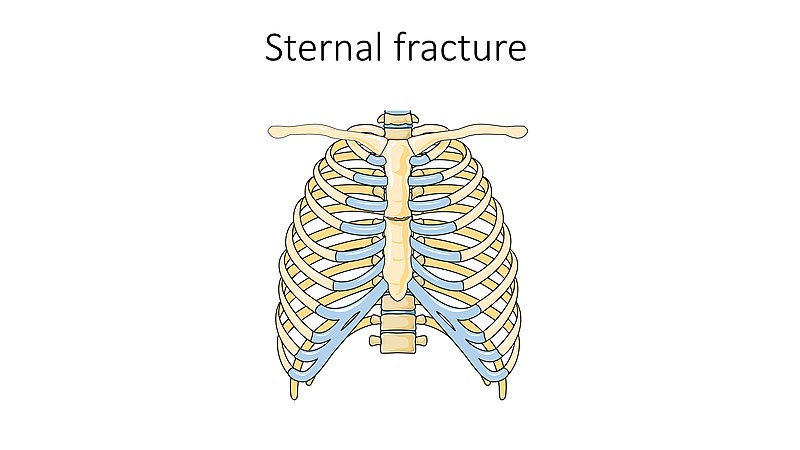
Sternal fractures are usually caused by anterior blunt chest trauma of the steering wheel as a result of motor vehicle accidents. Sternal fractures may cause vascular injury, as well as pulmonary and myocardial contusions. Electrocardiography and cardiac enzymes should be evaluated in sternal fractures. Rib fractures, pulmonary contusion, pneumothorax, hemothorax and even cranial injuries, spinal fractures and extremity traumas may associate with sternal fractures.
Fractures of the clavicle are quite common, accounting for up to 10% of all fractures. It is the most common fracture of childhood. A fall onto the lateral shoulder most frequently causes a clavicle fracture. The clavicle is an S-shaped bone and is the only osseous link between the upper extremity and the trunk. The clavicle articulates distally with the acromion at the acromioclavicular joint and articulates proximally with the sternum at the sternoclavicular joint. Due to its superficial subcutaneous location and the numerous ligamentous and muscular forces applied to it, the clavicle is easily fractured. Because the midshaft of the clavicle is the thinnest segment and does not contain ligamentous attachments, it is the most easily fractured location.
Commotio cordis is ventricular fibrillation precipitated by blunt trauma to the heart, not attributable to structural damage to the heart or surrounding structures. Its Latin etymology, “agitation of the heart,” describes the suspected mechanism whereby significant distortion of the myocardium creates enough mechanical energy to cause inappropriate depolarization, resulting in an unstable dysrhythmia.
Cases likely attributable to commotio cordis have been described for hundreds of years. Some of the earliest reports may relate to legends like Dim Mak, an ancient Chinese martial art technique to cause death by a carefully directed blow, christened “the touch of death.” Most cases currently reported involve young athletes playing sports.
