When A Stroke Doesn’t Look Like A Stroke
Published (updated: ).
Stroke Symptoms Are Based On The Location Of The Clot
At this point, medics should know that there are two main pathologies of stroke:
- Thrombotic Stroke – A blood clot is interrupting blood flow to downstream areas of the brain resulting in neurological symptoms.
- Hemorrhagic Stroke – A blood vessel in the brain has ruptured and is leaking somewhere inside the cranial vault. The neurological symptoms are also based on location. As the bleeding continues, the symptoms get worse due to increasing intracranial pressure. There is nothing like the decompensation of a cranial bleed.
The assessment that medics are taught is the Cincinnati Prehospital Stroke Scale. This easy to remember assessment is really only good at finding a left or right hemispheric stroke. What about the rest of the strokes?
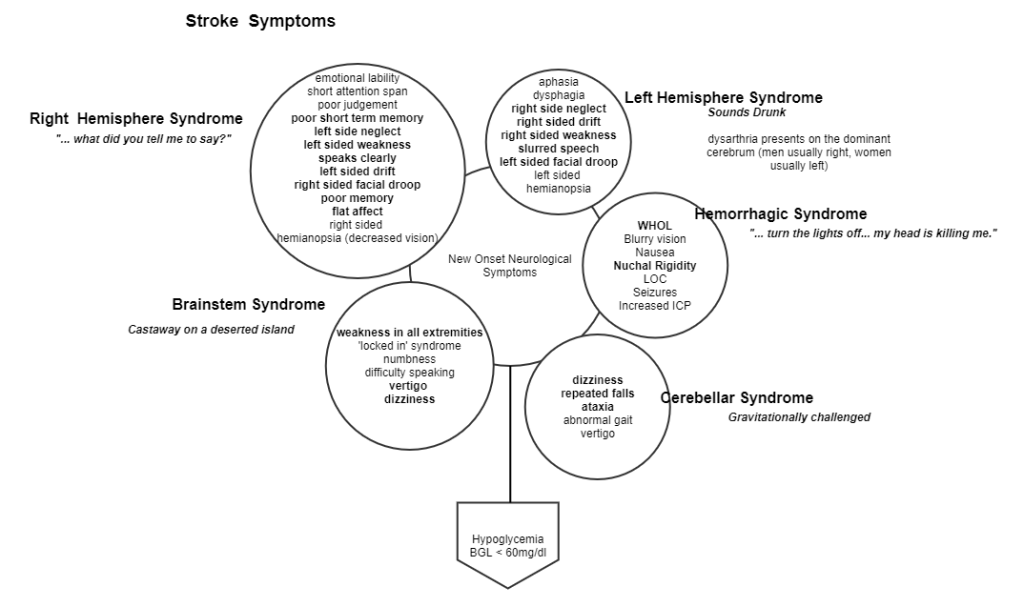
Stroke Syndromes Can Tell Us Where The Clot Is Located
- Right Hemispheric Stroke – Right hemisphere strokes tend to present with slurred speech or dysarthria (the patient is unable to speak in understandable sentences). A right hemisphere stroke may also increase the intensity of a patient emotions. Left arm drift and right facial flaccidity are also common.
- Left Hemisphere Stroke – Left hemisphere strokes tend to present with slurred speech, left facial flaccidity, and right arm drift.
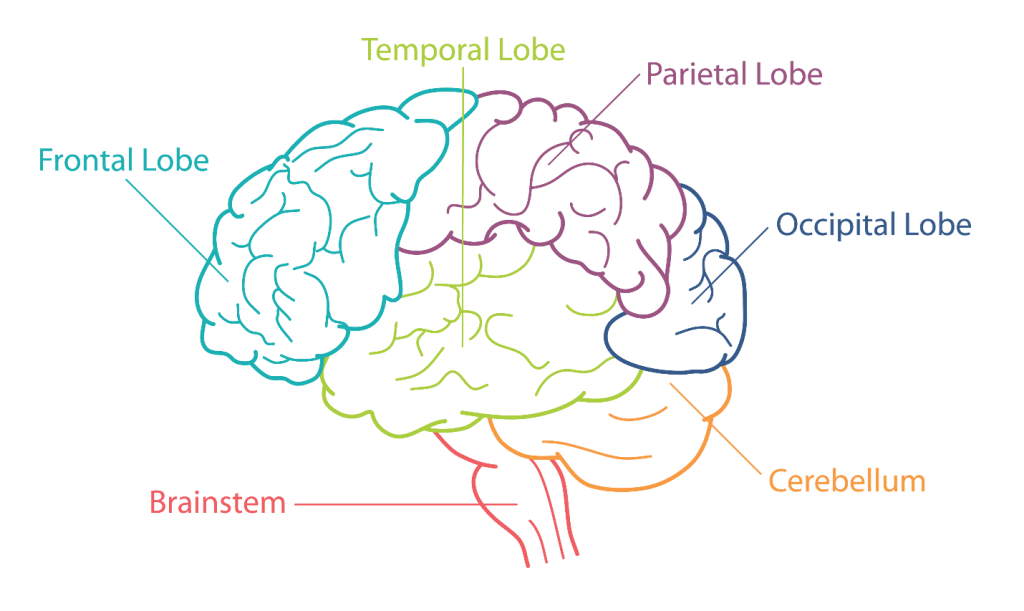
- Cerebellar Stroke – The cerebellum is a leaf shaped structure that connects the brain to the skull. The cerebellum is responsible for balance. When the cerebellum is injured, the patient will experience dizziness and may be unable to walk. Cerebellar strokes are typically dispatched as falls.
- Brainstem Stroke – Brainstem stroke is probably the hardest of all the strokes to pinpoint due to the fact that the patient is weak in all extremities. One could think of the brainstem stroke as a ‘whole body’ stroke. Unfortunately, these types of strokes are often discovered in the morning, well outside the established window of treatment (generally 3 hours from time of onset).
Hemorrhagic Strokes
Hemorrhagic strokes range from a terrible headache often referred to as the worst headache of life (WHOL). Hemorrhagic strokes are probably impossible for medics to distinguish from a severe headache. As the bleeding continues to increase intracranial pressure (remember, the bleeding is occurring in an intact skull), the patient may lose consciousness, vomit, or slowly become apneic.
The Common Thread
With all the variation in presentations of stroke, medics could become overwhelmed. Medics should consider the possibility of stroke anytime there is a new onset neurological deficit unexplained by blood glucose. Hypoglycemia is the greatest stroke mimic of all, however a glucometer makes distinguishing between hypoglycemia and a stroke fairly easy.
The Endgame
Medics should rapidly transport any patient with a suspected stroke to a stroke center for further evaluation. The stroke center has the ability to rule out hemorrhagic stroke and treat the patient with thrombolytics. Thrombolytics are drugs that dissolve blood clots, restoring circulation downstream of the clot and has the possibility of restoring neurological function back to normal in a matter of an hour. As risky as thrombolytic therapy can be, the alternative is physical therapy. At some point, the neurological damage caused by the clot is permanent and no amount of thrombolytics will improve the patient’s condition. In order to get the same response as thrombolytics, it may take as long as a year of physical therapy. Along the way, the patient’s disability often leads the patient to other problems such as injuries from falls and choking (stroke patients often have problems swallowing).
