START For Mass Casualty Triage
Published (updated: ).
The assessment that you will perform as a member of the triage team is simple. You will assess each patient in terms of respirations, pulse, and mental status. By virtue of this simple assessment, the medics should be able to determine (in less than 30 seconds) if a patient is dead/dying, immediate, or delayed. Remember, that patients who would have been tagged as minor are walking wounded (who are generally rounded up and put on a bus to a hospital).
| The RPM Assessment | |
| Respirations | Patients whose respirations are less than 30 are considered normal |
| Pulse | Patients with a radial pulse are considered normal |
| Mental Status | Patients who are awake and oriented are normal |
Everyone with respirations greater than 30 are abnormal or altered. Everyone without a radial pulse is abnormal or altered. Everyone who is unconscious or disoriented is considered abnormal. It’s that simple. The medics can refer to these patients as having an abnormal RPM. The only treatment that should be performed at an MCI is to open an airway (and, if necessary, insert an Oropharyngeal Airway) stop any visible bleeding (by handing the patient some 4×4’s), and elevate extremities for shock.
Using the RPM assessment tool, the triage team will classify patients in one of four categories:
| START Triage Categories | |
| Dead/Dying or ‘D’ | The DEAD/DYING are those who cannot breath after the airway is opened and are mortally wounded. These patients will probably die despite the best resuscitation efforts. An unconscious patient with agonal respirations can also be included in this category. It is often a difficult decision to leave a dying patient, especially if it is a child. But remember resources are often wasted here on unsalvageable victims. |
| Immediate or ‘C’ | IMMEDIATE patients are those who “RPM” is altered. Very simply, if a patient whose respirations (or R) is greater than 30, does not possess a radial pulse, or is disoriented or otherwise has an altered LOC. A patient can have 1 or all of the above conditions, These patient require immediate movement to the treatment or transport areas. In other words, patients without an intact RPM. |
| Delayed or ‘B’ | Patients who are unable to follow instructions to evacuate the scene, but who RPM is intact are categorized DELAYED. This is the most common category. It also includes patients who have a significant mechanism of injury, but whose RPM is intact. These patients can wait for treatment and/or transport until all the immediate’s are gone. |
| Minor or ‘A’ | MINOR patients are those at large incidents who were able to leave the impact area on the instruction of EMS personnel. These patients are referred to as the “walking wounded” and should be tagged later. These patients are the last priority. These patients will for treatment and/or transport until the immediate’s and delayed patients have been removed from the scene. |
Once triage is complete, a triage report should be radioed to dispatch. The first arriving company officer needs to quickly determine the most effective means to treat patients. In incidents with fewer patients, it may be more effective to treat patients “in place.” At EMS incidents with a greater number of patients, a treatment area should be established.
If there is a need for multiple triage teams, a triage officer will need to be assigned by the Incident Commander. The triage officer will be responsible for communicating the findings of the triage team to the transport team (a group of dedicated litter bearers who will move the patient to transport or treatment areas and ensuring accountability of the triage teams.
The idea behind triage is to sort, treat, and transport the greatest number of survivors in the shortest amount of time. Once a call of tremendous magnitude comes out, personnel from various other departments and ambulance services will drive miles out of their way to get to the incident.
If there are a lot of casualties, there are bound to be fatalities. One of the jobs of the Triage team is to identify the patients as fitting into one of four groups, dead, immediate, delayed, and minor. Just because there is a bunch of dead people lying around does not necessarily mean that the incident is over or has resolved itself. The events at the Tri-State Crematory in 2002 demonstrated a massive effort to collect all the bodies and properly identify them. One can extrapolate these events onto the scene of a large mass casualty incident. Like the hospitals, the incident may be also be duplicated through the eyes of the coroners who may have to manage hundreds of dead bodies.
Some events take months to resolve

Events of large geographic scale such as 9/11 or the New Orleans Flood took longer to resolve than a large motor vehicle crash. For the most part, a Mass Casualty Incident will be resolved in a matter of hours. If the incident requires a much larger scale and more time consuming operation, the incident will need to be expanded. When these incidents take longer to resolve, it will be necessary to summon additional resources and get them to the scene. The traditional role of Federal Emergency Management Agency (FEMA) at incidents has been to provide a bankroll for such long-term operations. When incidents reach a certain magnitude, it will be necessary to coordinate with the local Emergency Management Agency (EMA) as well as Georgia Emergency Management Agency (GEMA) to coordinate the delivery of additional personnel and equipment. Sometimes the additional support will come from other ambulance services in Georgia or other States. If the incident is large enough, the National Guard may be requested to provide assistance.
What happens next?
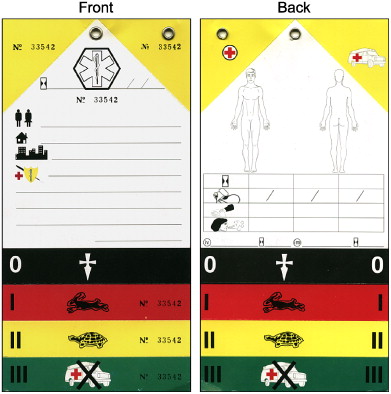
The entire incident has to be documented. The documentation includes patient care reports on each patient. Very often, the only documentation that will be available for each patient will be on the METTAG’s themselves. Collection of these tags may help aid in establishing exactly how many patients were treated, transport, or died.
At some point the rescuers will need to be debriefed about the incident. These debriefings may help investigators find the cause of the incident. The rescuers will need to discuss how they would improve should a similar incident occur in the future. The medics may need critical incident stress debriefing to discuss the emotional affects a call of this magnitude is likely to cause. Unfortunately, heroes (including medics) who live up to the tasks of a very difficult and stressful job have had a history of committing suicide to escape the horrible thoughts and dreams one would expect after a mass casualty incident.
