How To Look For Injuries
Published .
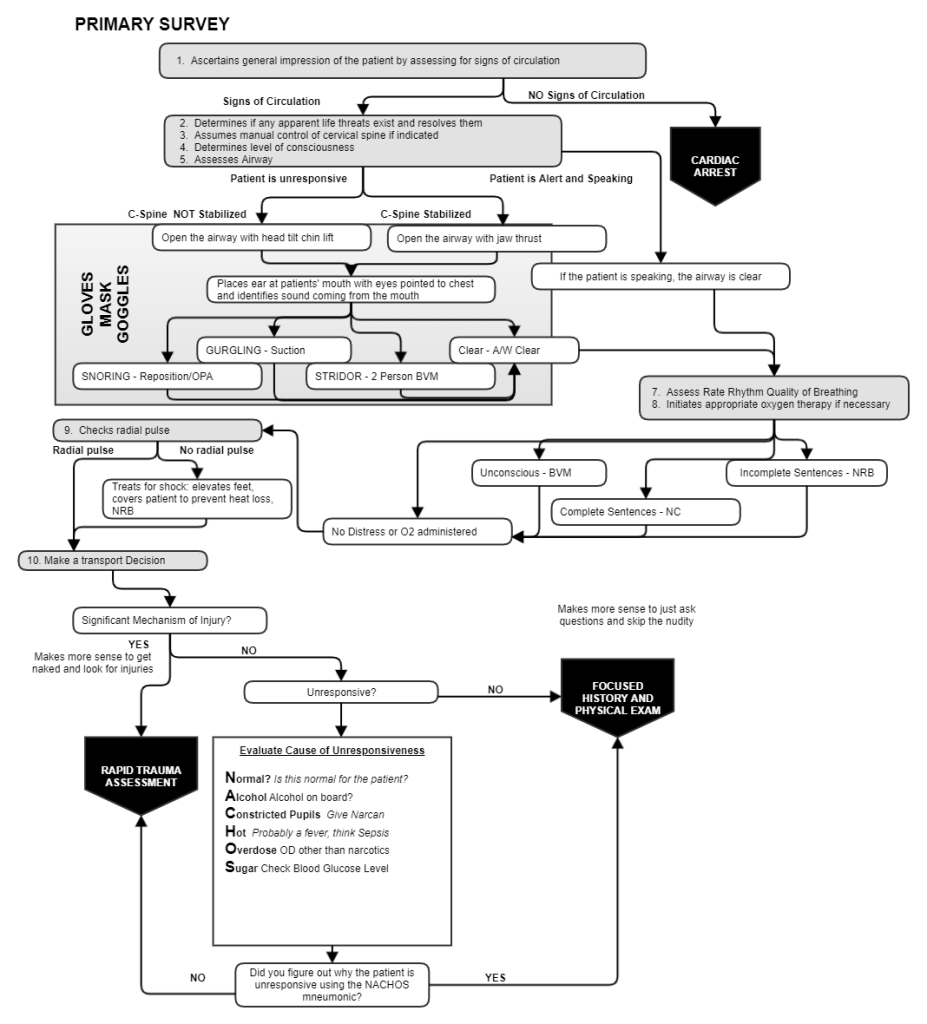
When a serious mechanism of injury is the cause of the patient’s condition or the patient is unresponsive for reasons unknown (after looking for an explanation of the loss of consciousness by using the NACHOS pneumonic), the ambulance crew needs to look for injuries. The EMS crew needs to look for injuries that could be made much more severe if they are not addressed before the patient is moved. Consider a broken femur. If the femur is moved without stabilization and ultimately splinted prior to being moved, the femur could tear the femoral artery and any tissues that surround the broken bone. It’s not specifically all injuries, but injuries that could be made worse by moving the patient to the ambulance.
Burns, Bleeding, Broken Bones
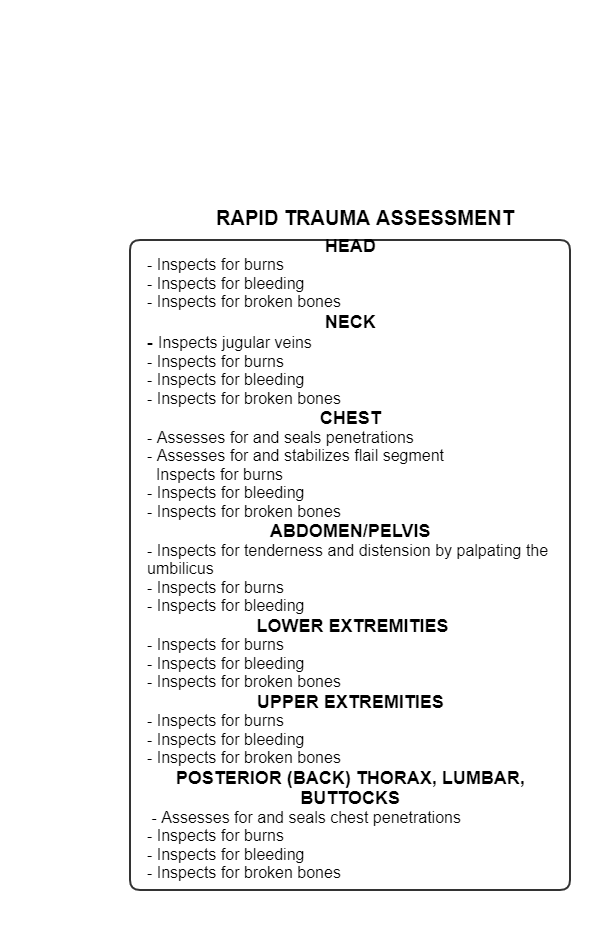
Looking for burns, bleeding, and broken can’t be performed with the patient wearing clothing. A patient could easily be experiencing serious bleeding under their clothes. This is why the ambulance crew has to cut off the clothes and inspect the patient’s body for burns, bleeding, and broken bones. It wouldn’t mean much to find these injuries if the medics didn’t have some idea how to treat them.
- Burns – Treating burns is easy. Expose the burn and cover the burn with a sterile burn sheet.
- Bleeding – Bleeding can be stopped by applying direct pressure. Other measures like tourniquets or wound packing may be necessary, but direct pressure is usually enough to stop most cases of bleeding. To stop bleeding with direct pressure, a rescuer applies some non sterile gauze over the wound and pushes down with their palm. Sometimes the bleeding doesn’t want to stop, so applying more pressure may be indicated. It may be necessary to apply this pressure to the wound for as long as 10 minutes (this may require the EMS crew to delegate the application of direct pressure to another member of the response team). In cases where bleeding won’t slow down or stop, a tourniquet may be applied.
- Broken bones – EMS is concerned with long bone fractures such as tibia/fibula, femur, ankles, wrists, radial/ulna, and humerus. The first step is to stabilize the broken extremity by having a rescuer simply keep it from moving. If the broken extremity is going to be splinted in the position of function, the extremity may be moved to the position of function during stabilization. Next the extremity is splinted with rigid splint and each joint above and below the extremity is immobilized. Stabilization and splinting can be delegated to other members of the response team.
Also look for important clues of life threatening injuries
In addition to finding and treating burns, bleeding, and broken bones, the medics can gain valuable insight about the patient’s condition by looking for clues to hidden injuries. The clues they should be looking for are:
- Jugular vein distension – This finding indicates the patient has a chest injury
- Penetrating wound to the chest – Most penetrating wounds are small, and require specific attention when looking for injuries. When the injury is found, the concern is that when the patient breathes, air will be sucked in through this hole in their chest and into their thoracic cavity (not necessarily their lungs). Sealing the wound with an occlusive dressing will greatly minimize the amount of air sucked into the lungs. This measure may also prevent a life threatening consequence to a penetrating wound to the chest; a tension pneumothorax.
- Flail chest – A flail chest is a condition where 2 or more ribs are broken in 2 or more places creating a floating ribcage. This floating ribcage is simply moving in the wake created by the intact ribs on the other side of the chest. This finding is called paradoxical respiration. Paradoxical respiration is treated by splinting the broken or floating ribs with a large bulky dressing.
- Abdominal rigidity or distension – This finding indicates that the patient has lost a considerable amount of blood in their abdomen. When a patient bleeds into their abdomen, the blood has left the vascular system, but remains in the body. Internal bleeding can easily be missed since there is no external bleeding to manage. The finding of abdominal distension or rigidity is an important finding that could explain why the patient is showing signs of shock.
The Rapid Trauma Assessment