Mechanical Airway Devices – OPA
Published (updated: ).
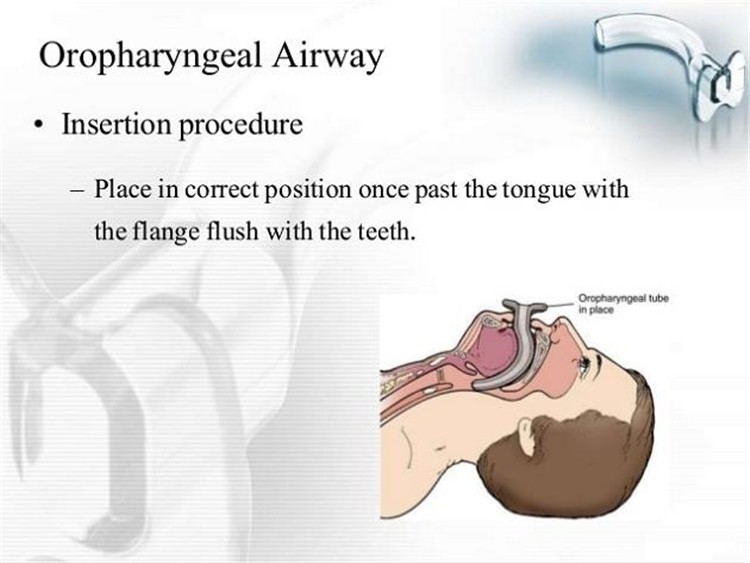
Oropharyngeal Airway

Indications
An oropharyngeal airway (oral airway, OPA) is an airway adjunct used to maintain or open the airway by stopping the tongue from covering the epiglottis. In this position, the tongue may prevent an individual from breathing. This sometimes happens when a person becomes unconscious because the muscles in the jaw relax causing the tongue to obstruct the airway.
Contraindications
Avoid using an oropharyngeal airway on a conscious patient with an intact gag reflex. If the patient can cough, they still have a gag reflex, and an oral airway is contraindicated. If the patient has a foreign body obstructing the airway, an oropharyngeal airway should not be used.
Preparation
An oropharyngeal airway has four parts: the flange, the body, the tip, and a channel to allow for passage of air and suction. Oropharyngeal airways come in a wide range of sizes (e.g., 40 mm to 110 mm). Choosing an appropriate oropharyngeal size is determined on an individual basis through the use of anatomical landmarks. When determining the appropriate oropharyngeal size for a patient, one must assess where the oropharyngeal airway parts lie in relation to the patient’s anatomical landmarks. The flange should be approximated, externally, to where it is abutting the lips, and the tip should be able to reach the angle of the mandible. Insertion of an oropharyngeal airway is not complicated but must be done with care to avoid further worsening of the airway obstruction, as well as, injuries to the airway.
Technique
There are several techniques, and the following are a few examples:
Technique 1: First, open the mouth. Then, using a tongue depressor, push down on the tongue and, with the tip pointed caudally, insert the oropharyngeal airway directly into the mouth over the tongue.
Technique 2: First, open the mouth. Then, with the tip pointed cephalad, insert the oropharyngeal airway into the mouth and then rotate it 180 degrees as it is advanced to the back of oropharynx. This technique carries the potential of injuring the hard and soft palates of the oral cavity.
Technique 3: First, open the mouth. Then, with the tip pointed at a corner of the mouth, insert the oropharyngeal airway into the mouth and then rotate it 90 degrees as it is advanced to the back of oropharynx.
Complications
Complications potentially caused by the use of oropharyngeal airways are that it may induce vomiting which may lead to aspiration. The gag reflex can be predicted if the patient has an intact eyelash reflex. To test the eyelash reflex, brush an eyelash with your finger. If the eyelid doesn’t move in response to the eyelash test, there probably is no gag reflex. Additionally, it may cause or worsen airway obstruction if an inappropriately sized airway is used (i.e., too small). An inappropriately sized airway can also cause laryngospasm (i.e., too big). Lastly, damage to the oral structures or dentition can also result from oropharyngeal airway insertion.

